The Great Fat Pad Migration of Metarsalgia
4 January 2026
By Mark Reyneker, B.T. Pod (SA), MSc (SA) Registered Podiatrist & Human Gait Specialist | Founder & Clinical Director, Family Podiatry Centre
The Evolution of Pathology: Atrophy vs. Migration
Structural Breakdown: Rupture and Exposure
Clinical Consequences and New Frontiers
Understanding this process and detecting it early is what we specialize in at the Family Podiatry Centre. We use EMED scanning equipment and gait analyses to trace changes that are occurring in the forefoot metatarsal area. For more on treatment read "Treating Metatarsalgia Caused By Fat Pad Pathology".
Book An Appointment
Disclaimer: The word "treatment" in this article refers to the care and management of a patient’s health to prevent, cure, or improve a condition. Treatment results vary and do not necessarily indicate a cure. This article is for informational and educational purposes only and does not constitute medical advice.
About the author
Mark Reyneker is a podiatrist and human gait specialist with 8 years of training and over 25 years of clinical experience. He is the Founder and Clinical Director of Family Podiatry Centre and has a Bachelors degree in Podiatric Medicine and a Master’s degree in paleoanthropology, with research focused on human foot function and metatarsal loading.
References:
Frequently Asked Questions
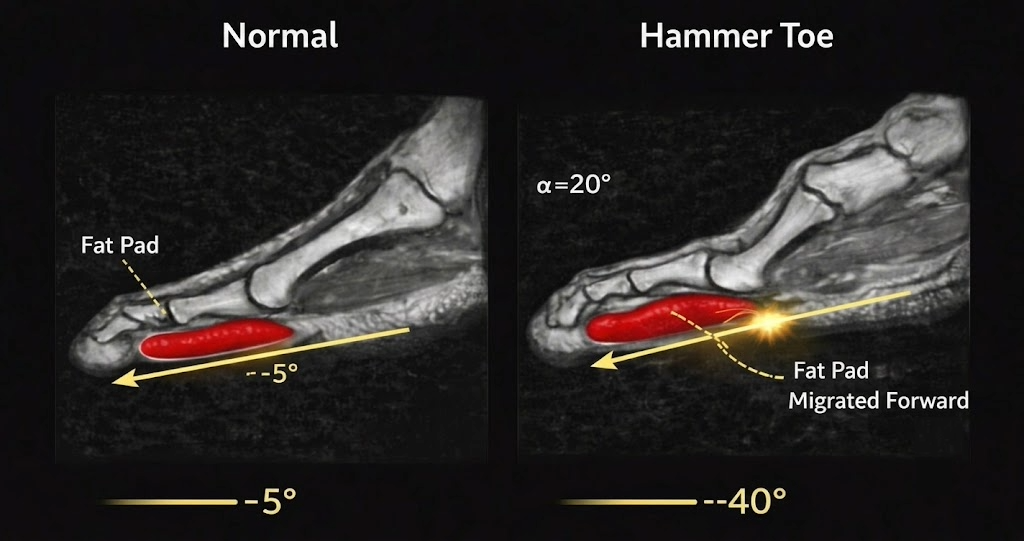
The plantar fat pad is anchored directly to the base of your toe bones (proximal phalanges). When toe deformities such as hammer toes or claw toes develop, the metatarsophalangeal (MTP) joint hyperextends and bends upward. This upward bend creates a "distal pull," mechanically dragging the protective fat cushion forward toward the toes and leaving the ball of the foot exposed.
Yes. In severe cases of toe deformity, MRI studies show that the distal pull becomes so intense that the fat tissue can rupture or separate completely in nearly 50% of deformed toes. This leaves the metatarsal head entirely unprotected against ground impact.
When toe deformities pull the fat pad forward, the protective padding under the metatarsal head drops dramatically from an average of 6.0 mm to just 2.5 mm. Meanwhile, the displaced padding under the toe bone increases from 7.6 mm to 9.1 mm, representing a 65% reduction in the overall thickness ratio between the ball of the foot and the toe.