Published: 28 June 2026 | Last reviewed: 29 June 2026
Retronychia is an under-recognised nail disorder in which the nail plate grows backwards or becomes embedded into the proximal nail fold — the skin fold at the base of the nail. Unlike the typical ingrown toenail, which usually affects the side of the nail, retronychia occurs at the back of the nail unit, near the cuticle and nail matrix. This makes it easy to miss, because patients often present with pain, swelling, redness, discharge, nail thickening, yellow nail discoloration, or apparent “infection” around the base of the nail.
The condition was first clearly described as a distinct clinical entity in the dermatology literature by de Berker and colleagues, who used the term retronychia to describe proximal ingrowing of the nail plate associated with stacked, misaligned nail plates beneath the proximal nail fold (de Berker et al., 2008). Since then, multiple case reports, retrospective studies, ultrasound studies and reviews have shown that retronychia is probably more common than once thought, but still frequently misdiagnosed as chronic paronychia, onychomycosis, ordinary onychocryptosis or traumatic nail dystrophy (Dahdah, Kibbi and Ghosn, 2008; Baumgartner and Haneke, 2010; Ventura et al., 2016; Litaiem et al., 2019).
For patients, the practical problem is simple: the toe hurts, the nail stops growing normally, the nail looks thick and yellow, and repeated courses of antibiotics or antifungal medication often do not solve the problem. For clinicians, the challenge is recognising that the primary problem is mechanical and structural — a disrupted nail plate has become trapped and driven into the proximal nail fold.
What is retronychia?
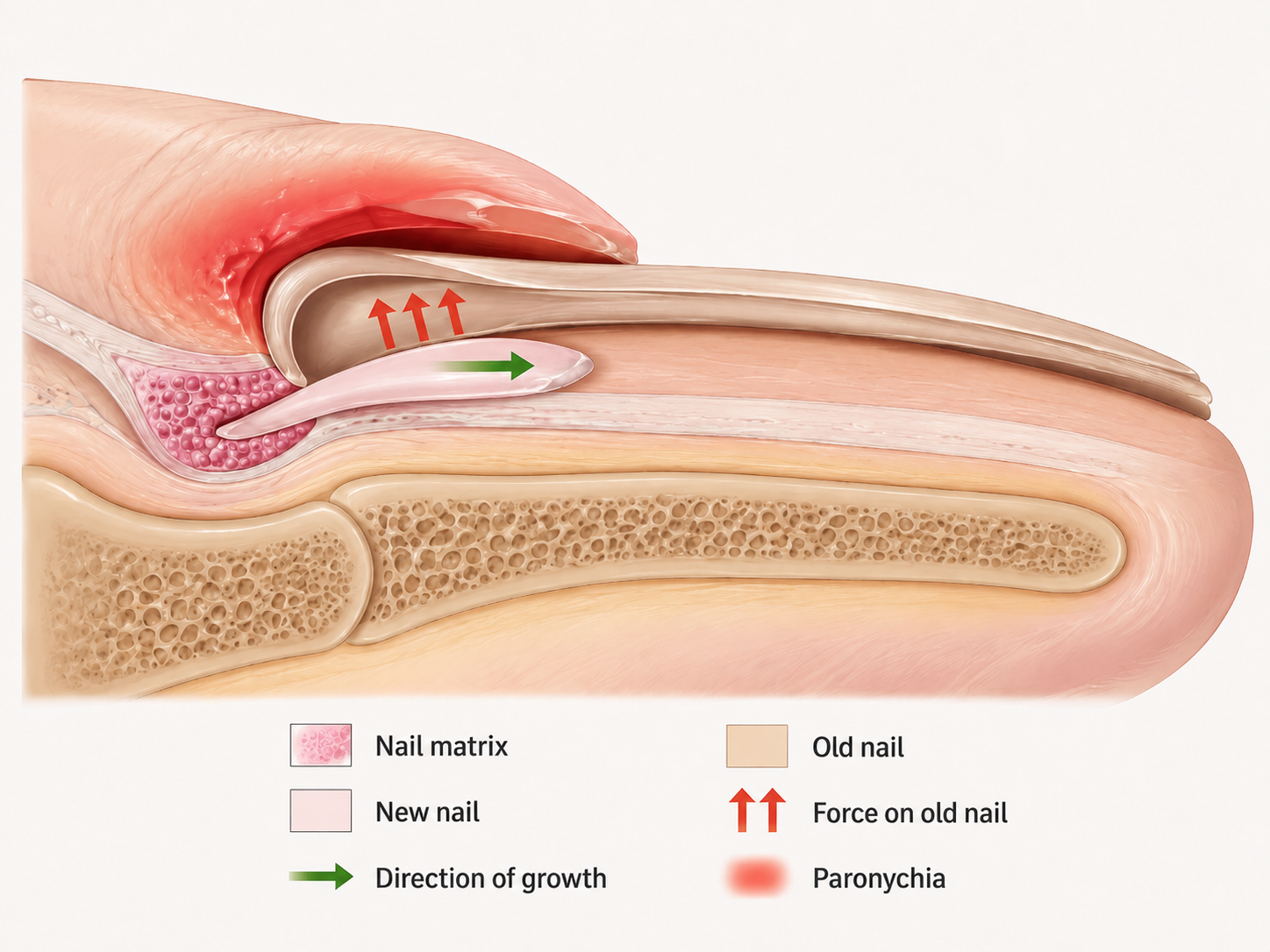
Retronychia refers to proximal ingrowth or embedding of the nail plate into the proximal nail fold. The word can be broken down as “retro”, meaning backwards, and “onychia”, relating to the nail. In simple terms, the nail does not simply grow forward as it should. Instead, after trauma or interruption of normal nail growth, the old nail plate may partially detach, the new nail plate forms beneath it, and the older nail plate is pushed upward and backward into the proximal nail fold (de Berker et al., 2008; Baumgartner and Haneke, 2010).
A useful way to understand this is to compare retronychia with onychomadesis. In onychomadesis, the nail matrix temporarily stops producing nail plate. The nail may later shed from the base. In many cases, the new nail grows beneath the old nail and pushes it forward. In retronychia, however, this process goes wrong. The old nail plate does not move forward normally. Instead, it becomes trapped under the proximal nail fold. Repeated cycles of nail plate production may then create multiple layers of nail stacked beneath the proximal fold (Wortsman et al., 2010; de Mello et al., 2018; Lencastre et al., 2024).
This explains several classic features of retronychia:
- The nail appears thickest proximally, near the base.
- The nail may look yellow, white-yellow, brown or dark.
- The nail may stop growing forward.
- The proximal nail fold becomes painful, swollen and inflamed.
- Granulation tissue may appear under the proximal fold.
- There may be discharge, but infection is often secondary or absent.
The condition is therefore not simply a “fungal nail” or a routine infection of the skin around the nail. It is a disorder of nail growth direction, nail plate layering and mechanical inflammation.
Book An AppointmentRelevant nail anatomy
To understand retronychia, it helps to review the anatomy of the nail unit.
The nail matrix is the growth centre that produces most of the nail plate. It sits beneath the proximal nail fold and extends partly under the visible pale crescent known as the lunula. The nail plate normally grows forward from the matrix and glides over the nail bed. The proximal nail fold protects the matrix and forms the skin fold at the base of the nail. The cuticle helps seal the space between the proximal nail fold and nail plate.
In a healthy toenail, the nail plate is produced by the matrix, remains aligned with the nail bed and moves forward gradually. In the big toenail, this process is slow. Toenails grow much more slowly than fingernails, so a disturbance to the toenail matrix may take many months to fully grow out.
In retronychia, the relationship between the nail matrix, nail plate and proximal nail fold is disrupted. Trauma may detach the nail plate from the matrix or nail bed. The older nail plate may then lose its normal forward movement. As the new nail plate develops, it may push the old plate upward and backward rather than forward. The sharp proximal edge of the older nail can then irritate or penetrate the underside of the proximal nail fold, causing persistent inflammation (Baumgartner and Haneke, 2010; Ventura et al., 2016).
Why does retronychia happen?
The dominant trigger in the literature is trauma. This can be an obvious direct injury, such as stubbing the toe, dropping something on the nail or a sports injury. More commonly, it may be repeated microtrauma from footwear, running, hiking, football boots, high heels, tight toe boxes, repetitive downhill walking or any activity that repeatedly drives the toe against the front of the shoe (de Berker et al., 2008; Gerard et al., 2016; Nagrani et al., 2019).
A common mechanism is repeated backward pressure on the distal nail plate. When the toe repeatedly hits the shoe, the nail may be pushed backward. If the nail plate partially detaches from the nail bed or matrix, normal forward nail growth may be interrupted. The new nail then grows beneath a partially detached old nail. If the old nail cannot move forward or shed normally, it becomes stacked and trapped proximally.
Reported risk factors include:
- Tight or poorly fitting footwear.
- High heels or shoes that push the toes forward.
- Running, tennis, hiking and other repetitive-impact sports.
- Direct toe trauma.
- Subungual haematoma.
- Distal onycholysis.
- Repeated nail manipulation.
- Previous nail surgery or trauma to the nail matrix.
- Foot deformity or altered toe loading.
- Pregnancy or postpartum physiological changes in some cases.
- Systemic illness or medication-associated nail matrix arrest.
- Chemotherapy, including reported cases following docetaxel.
- Cast immobilisation or altered limb use in rare cases.
(de Berker et al., 2008; Gerard et al., 2016; Baltz, Vatanchi and Jellinek, 2021; Kim et al., 2022; Alfaraj et al., 2025).
From a podiatric perspective, retronychia should not be viewed as an isolated nail disease only. It often reflects an interaction between the nail unit, footwear, activity load, trauma history and toe biomechanics.
Who gets retronychia?
Retronychia most often affects the great toenail. It can occur in fingernails, but toenails — especially the big toenails — are far more commonly involved because they are exposed to repetitive footwear pressure and ground-reaction forces (de Berker et al., 2008; Ventura et al., 2016; Litaiem et al., 2019).
Several studies suggest a predominance in women and young adults, although cases are reported in adolescents, older adults and men. The female predominance may partly reflect footwear factors, including narrow shoes and heels, but the condition is not limited to any one sex or age group (Dahdah, Kibbi and Ghosn, 2008; Gerard et al., 2016; Agharbi et al., 2023).
The clinical history often includes one of the following patterns:
- A painful big toenail after trauma.
- A nail that “stopped growing”.
- A chronically swollen proximal nail fold.
- A nail treated repeatedly as fungal without improvement.
- A recurrent “infection” at the base of the nail.
- A yellow, thickened nail that is worse at the base than the tip.
- A nail that became painful after increased running, hiking, sport or footwear change.
In the clinic, the most important clue is not simply the colour of the nail. It is the combination of proximal nail fold inflammation, interrupted nail growth and proximal nail plate thickening.
Clinical signs and symptoms
The classic clinical picture includes pain, swelling and inflammation at the proximal nail fold. This may look like chronic paronychia, but unlike typical paronychia, the inflammation is driven by abnormal nail plate position and mechanical irritation.
Common features include:
- Pain at the base of the nail.
- Tender swelling of the proximal nail fold.
- Redness or violaceous discoloration around the proximal nail fold.
- Yellow discoloration of the nail plate, known as xanthonychia.
- Thickening of the nail, especially proximally.
- Interrupted or absent forward nail growth.
- Onycholysis, where the nail separates from the nail bed.
- Beau’s lines or transverse grooves.
- Onychomadesis-like shedding.
- Granulation tissue emerging from beneath the proximal nail fold.
- Serous or purulent-looking discharge.
- Stacked layers of nail plate, sometimes only visible after avulsion.
(de Berker et al., 2008; Baumgartner and Haneke, 2010; Ventura et al., 2016; de Mello et al., 2018).
A particularly important feature is the mismatch between the apparent severity of “infection” and the poor response to antimicrobial treatment. Many patients receive antibiotics, antiseptic soaks or antifungal medication before the correct diagnosis is made. This happens because retronychia can look infectious, but the underlying driver is often mechanical embedding of the nail plate.
Early versus late retronychia
Clinically, retronychia can be thought of as early or advanced.
In early retronychia, the nail may show subtle growth arrest, mild proximal nail fold inflammation, yellow discoloration, discomfort and some exudate under the proximal fold. The nail may not yet show dramatic thickening or multiple obvious layers. These cases are easier to miss, but may respond better to conservative care if diagnosed early (Ventura et al., 2016; Laird, Lo Sicco and Rich, 2019; Sechi et al., 2022).
In advanced retronychia, the proximal nail fold inflammation is more intense, the proximal nail plate becomes thickened and elevated, granulation tissue may be visible, and multiple stacked nail plates may be present. At this stage, simple treatment for infection or fungus is unlikely to work. Nail plate avulsion is often required both to confirm the diagnosis and to relieve the mechanical conflict (Baumgartner and Haneke, 2010; Ventura et al., 2016; Sechi et al., 2022).
Recent reviews have also proposed more refined classifications, including acute, ongoing and chronic forms, but the practical clinical distinction remains whether the condition is early enough for conservative treatment or advanced enough to require avulsion (Lencastre et al., 2024; Alfaraj et al., 2025).
Why retronychia is often misdiagnosed
Retronychia is often misdiagnosed because its symptoms overlap with several common nail conditions.
Retronychia versus ordinary ingrown toenail:
A typical ingrown toenail, or onychocryptosis, usually affects the side of the nail. Pain, swelling and granulation tissue appear along the lateral nail fold. In retronychia, the problem is at the base of the nail, under the proximal nail fold. The nail grows or embeds backward rather than sideways.
Retronychia versus fungal nail infection:
Fungal nail infection can cause thickening, yellow discoloration, crumbling and onycholysis. Retronychia can also cause yellow thickening and onycholysis, so it may be mistaken for fungus. However, fungal nail disease usually does not cause marked painful proximal nail fold inflammation with arrested nail growth. Fungal testing may be needed if there is doubt, but a positive fungal culture does not always prove that fungus is the primary cause, because abnormal nails can become secondarily colonised.
Retronychia versus chronic paronychia:
Chronic paronychia is inflammation of the nail folds, often related to irritants, moisture exposure, barrier breakdown or inflammatory skin disease. Retronychia causes chronic-looking proximal nail fold inflammation, but the underlying driver is the embedded proximal nail plate. This is why chronic paronychia treatments may fail if the structural nail problem is not addressed.
Retronychia versus onychomadesis:
Onychomadesis is shedding of the nail from the proximal region due to nail matrix arrest. It may occur after systemic illness, fever, trauma, hand-foot-mouth disease or medication effects. Retronychia and onychomadesis are related because both involve disruption of nail matrix activity and nail plate growth. The difference is that in retronychia, the nail plate becomes proximally embedded and inflames the proximal nail fold rather than simply shedding forward (Wortsman et al., 2010; Wahlen et al., 2024).
Retronychia versus nail tumours or bone lesions:
Subungual exostosis, glomus tumour, mucous cyst, pyogenic granuloma, squamous cell carcinoma and other nail unit lesions can sometimes mimic inflammatory nail disease. Persistent pain, unusual pigmentation, a mass, bleeding, bone pain, progressive deformity or failure to respond to appropriate treatment should prompt further investigation. Ultrasound, radiography, biopsy or specialist referral may be required.
How retronychia is diagnosed
The diagnosis is primarily clinical. A careful history and nail examination are usually the most important tools.
Important questions include:
- Did the nail stop growing?
- Was there trauma, repeated shoe pressure or increased sport activity?
- Is the pain at the base of the nail rather than the side?
- Have antibiotics or antifungals failed?
- Is the proximal nail fold swollen or tender?
- Is the nail thickest near the base?
- Is there yellow discoloration, onycholysis or granulation tissue?
- Are there signs of multiple stacked nail plates?
Clinical diagnosis is supported by the combination of proximal nail fold inflammation, interrupted nail growth, proximal nail plate thickening and, in later cases, granulation tissue under the proximal fold (de Berker et al., 2008; Ventura et al., 2016).
The role of ultrasound
High-resolution ultrasound has become an important tool in confirming retronychia, especially when the diagnosis is uncertain. Ultrasound can show structural changes that are not obvious on visual inspection.
Reported ultrasound findings include:
- Two or more overlapping nail plates.
- Reduced distance between the origin of the nail plate and the base of the distal phalanx.
- Thickening of the proximal nail fold.
- Hypoechoic inflammatory changes around the proximal nail fold.
- Increased Doppler vascularity reflecting inflammation.
(Wortsman et al., 2010; Fernández, Reyes-Baraona and Wortsman, 2018; Arroyave et al., 2024).
Ultrasound is particularly useful when the differential diagnosis includes subungual tumour, cyst, exostosis, inflammatory arthritis or unusual onychomycosis. It can also help identify bilateral disease and guide whether conservative management is reasonable.
Treatment principles
The best treatment depends on the stage and severity of retronychia.
The core treatment goals are:
- Reduce mechanical trauma.
- Reduce inflammation.
- Restore normal nail growth direction where possible.
- Remove the embedded nail plate if conservative care is unlikely to work.
- Prevent recurrence by addressing footwear, activity load and toe mechanics.
Conservative treatment
Early or mild cases may be managed conservatively. Options reported in the literature include footwear modification, avoiding pressure on the affected nail, taping or adhesive techniques, clipping or reducing the onycholytic portion of nail, topical high-potency corticosteroids, intralesional corticosteroids in selected cases, and podiatric offloading or orthotic strategies where mechanical pressure is contributing (Ventura et al., 2016; Laird, Lo Sicco and Rich, 2019; Sechi et al., 2022).
Conservative treatment is most appropriate when:
- The condition is early.
- Pain is mild to moderate.
- There is no severe granulation tissue.
- The nail plate is not grossly stacked or elevated.
- There is no suspicion of tumour, osteomyelitis or severe infection.
- The patient can reduce the mechanical trigger.
In a retrospective study of conservative treatment, Laird, Lo Sicco and Rich (2019) reported conservative approaches in 25 patients, supporting the view that not every case requires immediate surgical avulsion. However, success depends heavily on correct case selection.
The 2022 systematic review by Sechi and colleagues found that conservative management was generally used for mild to intermediate disease, while avulsion was more commonly used for advanced cases. Their review also showed that there is no single standardised treatment pathway, which means clinical judgement remains essential (Sechi et al., 2022).
Nail plate avulsion
Nail plate avulsion remains the classic diagnostic and therapeutic treatment for advanced retronychia. Removing the nail plate allows the clinician to directly see the stacked nail plates and the sharp proximal nail edge responsible for the inflammation. It also removes the mechanical irritant from beneath the proximal nail fold (Baumgartner and Haneke, 2010; Ventura et al., 2016; de Mello et al., 2018).
Avulsion is usually considered when:
- Pain is significant.
- The proximal nail fold is persistently inflamed.
- Granulation tissue is present.
- The nail is markedly thickened proximally.
- Multiple nail plates are suspected.
- Conservative care has failed.
- Diagnosis remains uncertain and direct visual confirmation is needed.
Patients often experience rapid pain relief after the embedded nail plate is removed, although the nail itself takes months to regrow. The new nail may grow normally, but recurrence can occur if the underlying mechanical trigger persists.
Why antibiotics and antifungals often fail
Antibiotics and antifungals may be appropriate if there is confirmed bacterial infection or fungal infection. However, they do not correct the main mechanical problem in retronychia. This is why patients may report temporary or no improvement after multiple medication courses.
A toe with retronychia can look infected because the proximal nail fold is red, swollen, painful and sometimes draining. But this inflammation can be caused by the nail plate physically irritating the tissue from underneath. Treating only the secondary inflammation without addressing the embedded nail plate may delay proper care.
This is one of the most important educational messages for patients: a painful, yellow, inflamed nail is not always fungal and not always a simple infection.
Biomechanics and footwear considerations
From a podiatry perspective, retronychia should prompt questions about shoe fit, toe loading and activity.
Common contributing factors include:
A toe box that is too shallow.
A toe box that is too narrow.
Shoes that allow the foot to slide forward.
Long toenails repeatedly hitting the end of the shoe.
Running downhill.
Sports with sudden stopping.
High heels.
Foot deformity increasing pressure on the hallux.
Hallux limitus or altered propulsion.
Excessive pressure on the distal nail plate.
If the nail is repeatedly pushed backward in the shoe, the risk of recurrence may persist even after successful treatment. Patients should be advised to ensure adequate shoe length, adequate toe box depth, reduced pressure over the nail plate, and proper nail trimming. In athletes, training load, terrain and footwear choice may need review.
In some cases, orthoses or shoe modifications may help by reducing forward slide, improving foot stability or reducing excessive pressure through the hallux. The key is not simply to “remove the nail” but to understand why the nail was repeatedly traumatised in the first place.
When further investigation is needed
Further investigation should be considered when:
- There is severe pain disproportionate to the appearance.
- There is a visible or suspected mass.
- There is unusual pigmentation.
- There is recurrent bleeding.
- The nail deformity is progressive without trauma history.
- There is bone tenderness or suspicion of subungual exostosis.
- There is concern about osteomyelitis.
- The patient is immunocompromised or diabetic.
- The diagnosis is uncertain.
- There is no response to appropriate treatment.
Possible investigations include fungal microscopy and culture, bacterial culture if infection is suspected, ultrasound, X-ray, MRI in selected cases, or biopsy if a tumour or malignancy is a concern.
Prognosis
The prognosis is generally good when retronychia is recognised and treated appropriately. Advanced cases treated with nail plate avulsion often improve rapidly in terms of pain and inflammation. However, full cosmetic recovery depends on toenail regrowth, which can take many months.
The nail may regrow normally if the matrix is healthy and the mechanical cause is corrected. If there has been significant trauma, matrix scarring or persistent footwear pressure, the nail may remain thickened, ridged or dystrophic.
Recurrence prevention should focus on:
- Correct shoe fit.
- Avoiding repeated nail trauma.
- Managing sports-related toe pressure.
- Keeping nails trimmed appropriately.
- Addressing abnormal toe mechanics.
- Seeking early assessment if proximal nail fold pain returns.
Practical patient summary
Retronychia is a backward-growing or proximally embedded nail. It often affects the big toenail and commonly causes pain, swelling and inflammation at the base of the nail. It can look like a fungal nail, infected nail or ordinary ingrown toenail, but the problem is different. The nail plate becomes trapped under the proximal nail fold, sometimes with multiple layers of nail stacked on top of each other.
If a nail has stopped growing, become yellow and thick at the base, and the skin fold near the cuticle is painful or swollen, retronychia should be considered. Early cases may improve with pressure reduction, footwear changes and anti-inflammatory treatment. More advanced cases often require nail plate avulsion to remove the embedded nail and confirm the diagnosis.
Conclusion
Retronychia is a clinically important nail condition because it is painful, commonly misdiagnosed and often treated incorrectly before the true cause is recognised. The hallmark is not simply a thick yellow nail, but the combination of proximal nail fold inflammation, arrested nail growth and proximal nail plate embedding.
For patients, awareness matters because repeated antibiotics or antifungal treatments may not solve the problem. For clinicians, recognising retronychia early allows more appropriate treatment, avoids unnecessary medication, and may prevent months of persistent pain.
The condition sits at the intersection of dermatology, podiatry, nail surgery, footwear mechanics and trauma medicine. A careful history, close nail examination, and ultrasound where needed can make the diagnosis clearer. Treatment should be matched to severity: conservative offloading and anti-inflammatory care for early disease, and nail plate avulsion for advanced or persistent cases.
Book An Appointment
Disclaimer: The word "treatment" in this article refers to the care and management of a patient’s health to prevent, cure, or improve a condition. Treatment results vary and do not necessarily indicate a cure. This article is for informational and educational purposes only and does not constitute medical advice.
About the authorMark Reyneker is a podiatrist and human gait specialist with 8 years of training and over 25 years of clinical experience. He is the Founder and Clinical Director of Family Podiatry Centre and has a Bachelors degree in Podiatric Medicine and a Master’s degree in paleoanthropology, with research focused on human foot function and metatarsal loading.
References
2.
Alfaraj, M.M., Mohammed, A., Aljabr, Z.A., Alsaleh, A.K., Al-Ghanem, S.K., Alotaibi, S.A., Alammar, J.O. and Al Breiki, S.A. (2025) ‘Retronychia: a comprehensive review of etiologies, clinical manifestations, diagnostics, and management’, Electronic Journal of General Medicine, 22(6), em692.
6.
de Berker, D.A.R., Richert, B., Duhard, E., Piraccini, B.M., André, J. and Baran, R. (2008) ‘Retronychia: proximal ingrowing of the nail plate’, Journal of the American Academy of Dermatology, 58(6), pp. 978–983.
8.
Gerard, E., Prevezas, C., Doutre, M.S., Beylot-Barry, M. and Cogrel, O. (2016) ‘Risk factors, clinical variants and therapeutic outcome of retronychia: a retrospective study of 18 patients’, Journal of the European Academy of Dermatology and Venereology, 30(4), pp. 640–642.
11.
Litaiem, N., Drissi, H., Zeglaoui, F. and Khachemoune, A. (2019) ‘Retronychia of the toenails: a review with emphasis on pathogenesis, new diagnostic and management trends’, Archives of Dermatological Research, 311(7), pp. 505–512.13. Ventura, F., Correia, O., Duarte, A.F., Barros, A.M. and Haneke, E. (2016) ‘Retronychia: clinical and pathophysiological aspects’, Journal of the European Academy of Dermatology and Venereology, 30(1), pp. 16–19.
15.
Zaraa, I., et al. (2012) ‘Retronychia: a rare cause of chronic paronychia’, Dermatology Online Journal, 18(6), p. 9.16.
Baltz, J.O., Vatanchi, M. and Jellinek, N.J. (2021) ‘Retronychia triggered by docetaxel’, Dermatologic Surgery, 47(6), pp. 884–885. 17.
Fernández, J., Reyes-Baraona, F. and Wortsman, X. (2018) ‘Ultrasonographic criteria for diagnosing unilateral and bilateral retronychia’, Journal of Ultrasound in Medicine, 37(5), pp. 1201–1209.18.
Wortsman, X., Wortsman, J., Guerrero, R. and Soto, R. (2010) ‘Anatomical changes in retronychia and onychomadesis detected using ultrasound’, Dermatologic Surgery, 36(10), pp. 1615–1620.19.
Sechi, A., et al. (2022) ‘Treatment of retronychia: a systematic review and suggested treatment algorithm’, Dermatologic Therapy, 35(1), e15251.