Can Footwear and Insoles Help with Medial Knee Osteoarthritis?
23 April 2026
Knee osteoarthritis is one of the most common causes of chronic pain, reduced walking tolerance and loss of independence in middle-aged and older adults. In everyday practice, the most important non-surgical treatments remain education, exercise therapy, weight management where appropriate, and sensible symptom control. Footwear and foot orthotics sit in a different category: they are adjunctive load-modifying tools, not a replacement for core osteoarthritis care. That distinction matters, because the literature shows a stronger effect on knee mechanics than on pain and function. In other words, an insole may reduce the forces associated with medial compartment loading without reliably making every patient feel better. (Kolasinski et al., 2020; American Academy of Orthopaedic Surgeons, 2021).
For doctors, that means the right question is not simply, “Do lateral wedge insoles work?” The better question is, “In which patient, for which compartment pattern, and with what orthotic design, can footwear meaningfully improve loading and symptoms?” For patients and families, the same point can be stated more simply: a shoe or insole may help some knees, but it is rarely a universal fix.
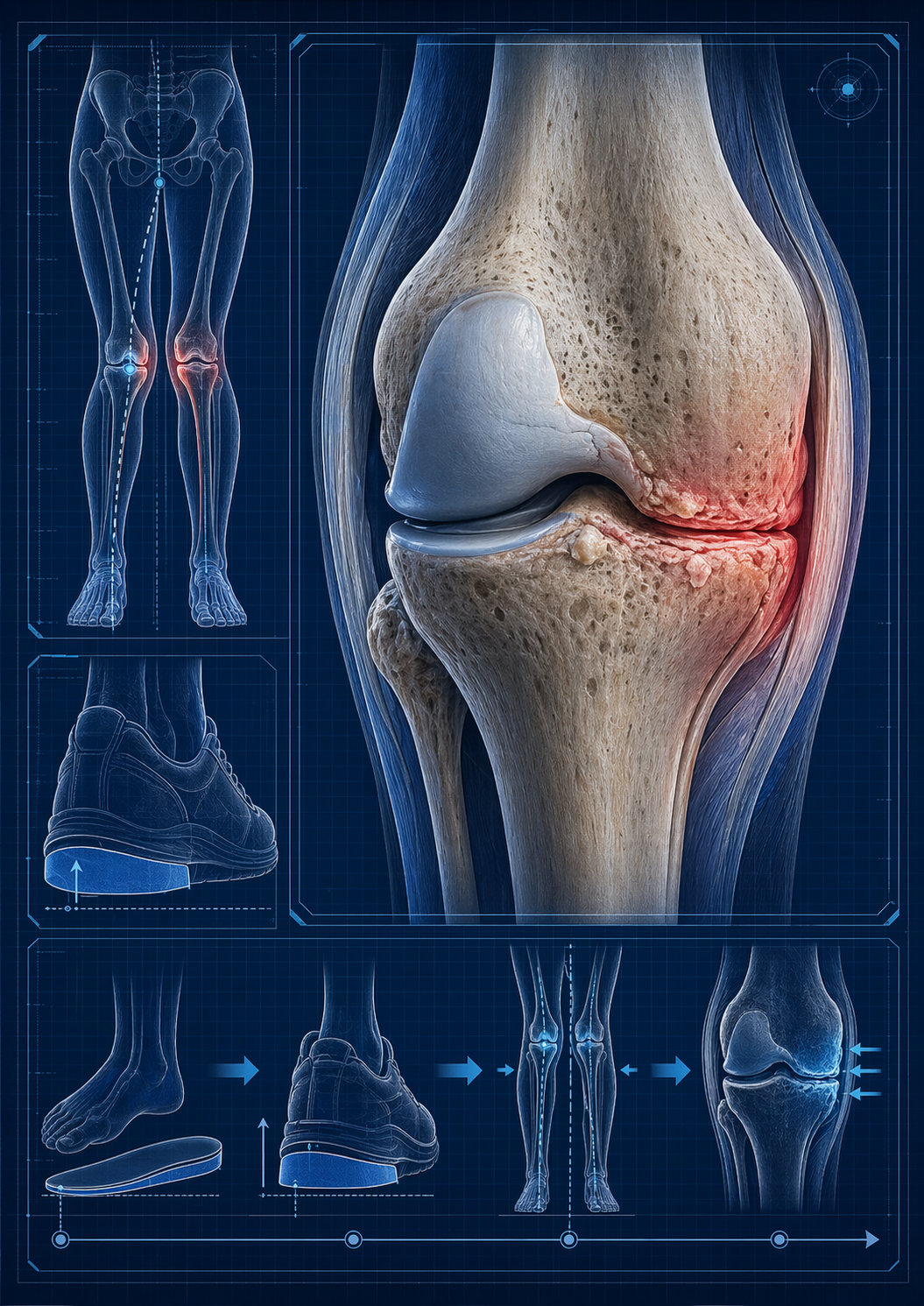
Why the medial compartment is such a focus
Most symptomatic tibiofemoral knee OA affects the medial compartment. In many of these patients, walking generates a frontal-plane loading pattern that tends to compress the inside of the knee more than the outside. Researchers commonly study this using the external knee adduction moment (EKAM) and the knee adduction angular impulse (KAAI). These are not direct measurements of cartilage stress, but they are widely used biomechanical surrogates for medial compartment loading during gait. This is why so much of the footwear literature focuses on ways of reducing EKAM rather than simply changing comfort alone (Arnold et al., 2016; Hinman et al., 2012).
How a lateral wedge is supposed to work
A lateral wedge insole places the foot in relative valgus by elevating the lateral side of the foot. The intended effect is to shift the center of pressure laterally and shorten the frontal-plane lever arm of the ground reaction force relative to the knee. In practical terms, that may reduce the adduction moment acting across the knee during stance. Early clinical biomechanics papers helped establish this principle. Kerrigan and colleagues showed that lateral wedges reduced knee varus torque during walking in people with knee OA, while Kakihana and colleagues showed that a lateral wedge could reduce knee varus moment while increasing subtalar valgus moment, helping explain the foot-to-knee mechanical chain (Kerrigan et al., 2002; Kakihana et al., 2005).
Hinman and colleagues strengthened this mechanistic argument in medial knee OA by showing that lateral wedges reduced peak KAM and that much of the effect seemed to come from reducing the knee-to-ground-reaction-force lever arm. In short, the orthosis does not “heal” the arthritic compartment; it attempts to alter the line of force through the limb during gait (Hinman et al., 2012).
What the supportive biomechanical studies show
The mechanical literature is reasonably consistent. Several studies have shown that lateral wedges can reduce medial knee loading during level walking. Kerrigan et al. demonstrated reduced knee varus torque with 5° and 10° wedges. Kakihana et al. showed reduced knee varus moment and linked this to altered subtalar mechanics. Hinman et al. showed an immediate reduction in KAM with lateral wedges in medial knee OA, and later showed that this load-reducing effect did not appear to degrade after a month of wear, arguing against the idea that wedge compression rapidly eliminates the intervention’s mechanical effect (Kerrigan et al., 2002; Kakihana et al., 2005; Hinman et al., 2008; Hinman et al., 2009).
The same offloading signal has been observed in more demanding functional tasks. Alshawabka et al. reported that lateral wedges reduced medial compartment loading during both stair ascent and descent, including first and second peak EKAM and KAAI. That matters clinically because stairs are often one of the first tasks that provoke knee OA pain and functional complaint (Alshawabka et al., 2014).
When the literature is pooled, the same message remains: small but statistically significant improvements in biomechanical load measures are seen on average. Arnold et al. concluded that lateral wedge insoles produce small reductions in biomechanical risk factors associated with medial knee OA progression, and Xing et al. similarly found pooled reductions in first-peak EKAM, second-peak EKAM and KAAI in patients with medial knee OA. These reviews are useful because they confirm that the mechanical concept is real, even if the clinical benefit is not uniform (Arnold et al., 2016; Xing et al., 2017).
Why the clinical outcome story is more mixed
This is where a doctor-facing article has to be honest. A reduction in EKAM does not automatically mean meaningful pain relief. Bennell et al. performed one of the most important longer-term trials and found that lateral wedge insoles worn for 12 months provided no symptomatic or structural advantage over flat control insoles. Parkes et al., in a meta-analysis published in JAMA, likewise concluded that lateral wedge insoles were not efficacious for pain reduction when compared with appropriate controls (Bennell et al., 2011; Parkes et al., 2013).
That difference between load reduction and symptom reduction is not theoretical. Jones et al. found that even when lateral wedges reduced EKAM, the degree of mechanical change did not clearly track with immediate pain change. In other words, some biomechanical responders were not clinical responders, and vice versa. Pain in OA is influenced by much more than frontal-plane joint loading alone: synovial irritation, bone marrow lesions, neuromuscular strategy, patellofemoral involvement, walking speed, fear, and general deconditioning all matter (Jones et al., 2014).
So are orthotics useless? No. They are probably selective tools.
The most sensible interpretation is not that lateral wedges “do not work,” but that routine, one-size-fits-all prescription is weakly supported. The better evidence points toward individualization. Felson et al. addressed this directly by prescreening patients to exclude those with patellofemoral OA and those who did not demonstrate a biomechanical response. In that more carefully selected group, lateral wedges produced a statistically significant, though small, reduction in pain compared with neutral insoles. The effect size was modest, but the paper is important because it supports the idea that patient selection matters (Felson et al., 2019).
Hunt et al. offer another useful clue. In patients with medial knee OA and pronated feet, adding a custom arch support to a 5° lateral wedge improved timed stair performance, reduced knee and foot symptoms within condition, and was preferred by more participants than the wedge alone. This suggests that orthotic design should not be reduced to “just add a wedge.” Foot posture, comfort, tolerance and the interaction between rearfoot control and knee mechanics matter (Hunt et al., 2017).
What about footwear rather than insoles alone?
Footwear itself also influences knee loading, but again the clinical literature is mixed. Hinman et al. tested “unloading shoes” with modified midsoles designed to reduce medial knee load and found that they provided no additional benefit over conventional walking shoes, even though both groups improved in pain and function over time. Paterson et al. later compared flat flexible shoes with stable supportive shoes in people with symptomatic medial knee OA and found that flat flexible shoes were not superior; stable supportive shoes actually improved walking pain more, and adverse events were fewer in the stable supportive group (Hinman et al., 2016; Paterson et al., 2021).
For clinicians, this is an important corrective. A mechanically attractive concept such as “more barefoot-like” or “more flexible” does not automatically produce better outcomes in a symptomatic OA population. Comfort, stability, tolerance, daily-use practicality and the patient’s broader movement pattern still matter.
Where footwear and orthotics fit in modern non-surgical management
Current guideline language reflects this nuance. The 2019 ACR/Arthritis Foundation guideline stated that the available literature does not demonstrate clear efficacy for lateral or medial wedged insoles. The 2021 AAOS guideline went further and stated that lateral wedge insoles are not recommended for patients with knee osteoarthritis as a routine treatment. These recommendations do not invalidate the biomechanics literature; they simply recognize that the average clinical benefit across unselected patients has not been convincing enough for blanket endorsement (Kolasinski et al., 2020; American Academy of Orthopaedic Surgeons, 2021).
That means orthotics should usually be presented as an adjunctive option within a broader conservative program that still prioritizes strengthening, walking capacity, weight management where relevant, activity modification, and sensible analgesic or anti-inflammatory strategies when indicated. This is especially important in referral conversations, because an insole should not be oversold as a stand-alone treatment for established OA.
Which patients may still be reasonable candidates for podiatric referral?
A podiatric or orthotic referral is most defensible when the patient has symptomatic medial tibiofemoral OA, especially where there is clinical suspicion of varus-driven loading, pain aggravated by walking or stairs, a potentially modifiable foot posture, footwear intolerance, or a desire to trial conservative load modification before bracing or surgery. Patients with pronated feet may be especially relevant when a supported lateral wedge rather than a simple wedge is being considered (Hunt et al., 2017; Felson et al., 2019).
For patients and families, the practical message is straightforward. An orthotic trial may be worth considering when pain seems related to everyday loading, but it should be assessed like any other treatment: Does walking feel better? Are stairs easier? Is comfort acceptable? Can the device be worn consistently? A mechanically elegant device that sits in the shoe drawer is not an effective treatment.
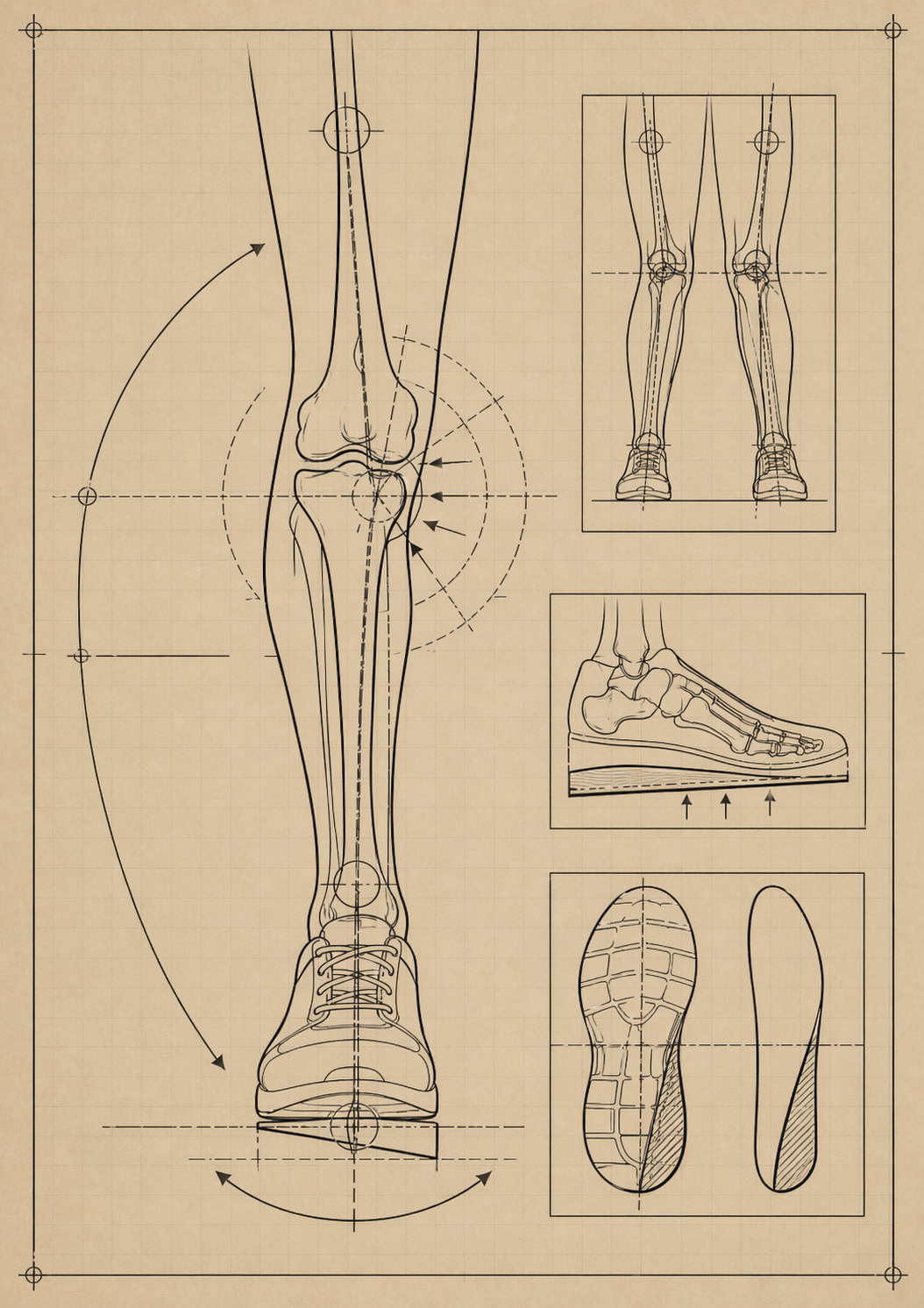
What a proper assessment should include
A meaningful footwear/orthotic assessment for knee OA should go beyond simply handing the patient a generic wedge. At minimum, it should consider the painful compartment pattern, frontal-plane knee alignment, shoe type, foot posture, tolerance at the foot and ankle, and whether symptoms worsen on stairs, hills or prolonged walking. Where possible, dynamic gait assessment is useful because OA patients are heterogeneous: some clearly offload with wedges, some do not, and some may shift load in ways that are mechanically or symptomatically unhelpful (Hinman et al., 2012; Jones et al., 2014; Felson et al., 2019).
In a specialist podiatry setting, that may mean trialling a lateral wedge alone, a lateral wedge with arch support, or a shoe-based modification rather than assuming one format suits all. The goal is not merely to change an abstract gait variable, but to find a configuration that is comfortable, wearable and clinically useful.
The practical bottom line
The literature supports the idea that footwear and foot orthotics can alter knee mechanics in medial knee OA. Lateral wedges can reduce medial knee loading during walking, and supported wedge designs may improve tolerance and sometimes function in selected patients. However, the best clinical trials do not support routine prescription for all patients, and major guidelines now recommend against using lateral wedge insoles as a blanket treatment. The most defensible modern position is this: footwear and orthotics are individualized adjuncts, not universal solutions. They are most valuable when prescribed selectively, fitted properly, and integrated into a broader non-surgical OA strategy.
For referring doctors, that makes podiatric referral reasonable not because every medial knee OA patient needs a wedge, but because some patients benefit from a carefully assessed load-modification trial that includes footwear review, orthotic design and functional follow-up. For patients, it means there is a conservative option worth exploring, provided expectations remain realistic and treatment is individualized.
Disclaimer: The word "treatment" in this article refers to the care and management of a patient’s health to prevent, cure, or improve a condition. Treatment results vary and do not necessarily indicate a cure.
Disclaimer: The word "treatment" in this article refers to the care and management of a patient’s health to prevent, cure, or improve a condition. Treatment results vary and do not necessarily indicate a cure.
References
13. Xing, F., Lu, B., Kuang, M.J., Wang, Y., Zhao, Y.L., Zhao, J. et al. (2017) ‘A systematic review and meta-analysis into the effect of lateral wedge arch support insoles for reducing knee joint load in patients with medial knee osteoarthritis’, Medicine, 96(24), e7168. doi: 10.1097/MD.0000000000007168.
14. Hinman, R.S., Bowles, K.A. and Bennell, K.L. (2009) ‘Laterally wedged insoles in knee osteoarthritis: do biomechanical effects decline after one month of wear?’, BMC Musculoskeletal Disorders, 10, p. 146. doi: 10.1186/1471-2474-10-146.
Written and prepared by:
Mark Reyneker
14. Hinman, R.S., Bowles, K.A. and Bennell, K.L. (2009) ‘Laterally wedged insoles in knee osteoarthritis: do biomechanical effects decline after one month of wear?’, BMC Musculoskeletal Disorders, 10, p. 146. doi: 10.1186/1471-2474-10-146.
Written and prepared by:
Mark Reyneker
B.T. Pod (SA), MSc (SA)
Podiatrist and Human Gait Specialist
Registered with the Podiatry Association of Singapore
Founder and Director:
Family Podiatry Centre Pte Ltd
Family Podiatry Centre Sdn Bhd
Solescape Orthotics Laboratory
Solescape Shoes brand