Leg Length Discrepancy: Why Even Small Differences Can Matter
7 June 2026
By Mark Reyneker, B.T. Pod (SA), MSc (SA) Registered Podiatrist & Human Gait Specialist | Founder & Clinical Director, Family Podiatry Centre
Published: 7 June 2026 | Last reviewed: 8 June 2026
Many people are told that a small leg length difference is “normal” or “not a problem unless it is more than 1 cm”. That statement is incorrect. A small difference in leg length may not matter in one person, but it can matter a great deal in another person if it creates asymmetrical loading, pelvic compensation, recurrent pain, gait changes, or overuse injury.
What is leg length discrepancy?
Leg length discrepancy, often shortened to LLD, means that one leg functions as shorter than the other. There are two main types.
The first is structural or anatomical LLD. This means there is a true difference in the bony length of the limbs. For example, one femur or tibia may be slightly shorter than the other. This can occur naturally, after childhood growth variation, previous fracture, joint disease, hip or knee replacement, or other developmental or surgical causes.
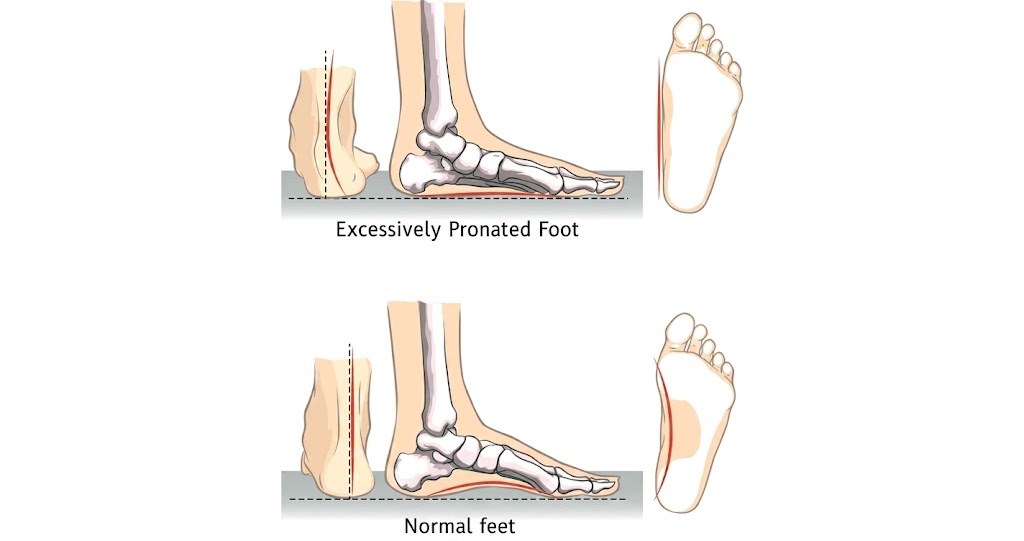
The second is functional LLD. This means the legs may be similar in actual bone length, but the body behaves as if one leg is shorter. This may happen because of pelvic tilt, scoliosis, hip tightness, knee flexion, ankle equinus, foot posture, pronation, supination, muscle imbalance, or compensatory movement patterns.
In real clinical practice, patients often have a mixture of both. This is one reason leg length discrepancy is controversial: measuring the bones alone does not always explain how the person actually walks, stands, loads the feet, or experiences symptoms.
Alfuth, Fichter and Knicker’s systematic review found that measurement methods vary considerably, but the block test is one of the more useful clinical screening methods, while full-length standing radiography is considered a strong imaging reference for anatomical LLD (Alfuth et al., 2021).
Alfuth, Fichter and Knicker’s systematic review found that measurement methods vary considerably, but the block test is one of the more useful clinical screening methods, while full-length standing radiography is considered a strong imaging reference for anatomical LLD (Alfuth et al., 2021).
Why the old “less than 1 cm is fine” rule is not good enough
The old orthopedic threshold of 1 cm is largely a surgical threshold, not a functional threshold. In other words, it may be reasonable to say that a 5–8 mm discrepancy is not usually a surgical problem. It is not reasonable to automatically conclude that it is not a biomechanical problem.
This distinction matters. A small discrepancy may be repeated through thousands of steps per day. A person who walks 8,000 steps daily exposes the body to millions of loading cycles each year. In a runner, athlete, nurse, teacher, chef, surgeon, hairdresser, retail worker, or anyone who stands for long periods, small asymmetries may accumulate.
Rannisto et al. found that workers with standing jobs and LLD of 5 mm or more were eligible for a randomized controlled trial of insole correction; their study concluded that LLD of 5 mm or more “seems to be worth correcting” in people with standing jobs and low back pain (Rannisto et al., 2019).
This does not mean every 5 mm discrepancy must be treated. It means it should not be dismissed when the symptoms and examination fit.
How common is leg length discrepancy?
Small differences in leg length are common. That is part of the reason the topic is confusing. If many people have some degree of asymmetry, then asymmetry alone cannot be the whole diagnosis.
The key is to distinguish between:
a harmless finding,
a contributing factor, and
a primary mechanical driver of symptoms.
a contributing factor, and
a primary mechanical driver of symptoms.
The literature suggests that LLD is common and that there is no universal agreement on what degree should be considered clinically significant. Pereiro-Buceta et al. noted that LLD has been controversial because of disagreement around prevalence, measurement, clinical significance and association with musculoskeletal disorders (Pereiro-Buceta et al., 2021).
A useful clinical approach is to evaluate if the difference is relevant to symptoms or affects the leg and foot loading patterns.
How small leg length discrepancies can affect the body
1. Pelvic tilt and spinal compensation
When one leg functions shorter than the other, the pelvis may drop or rotate. The spine may then compensate above the pelvis. Some patients feel this as low back ache, sacroiliac discomfort, hip tightness, or a sense that they are “standing crooked”.
D’Amico, Kinel and Roncoletta studied patients with nonspecific low back pain and LLD using 3D stereophotogrammetric posture analysis. They found that customized heel-lift orthotics with full LLD correction were associated with improved postural parameters and marked pain reduction over medium- and long-term follow-up (D’Amico et al., 2022).
The important clinical message is not that every back pain case is caused by LLD. It is that in selected patients, LLD can be part of the mechanical chain.
2. Changes in foot pressure and gait timing
A leg length difference does not only affect the pelvis and back. It also affects how the feet load the ground.
Pereiro-Buceta et al. tested simulated LLD in healthy subjects using a pressure platform. As the simulated discrepancy increased, the long leg showed reduced mean and peak pressure, while the short side became relatively overloaded; the long leg also showed increased stance time (Pereiro-Buceta et al., 2021).
O’Toole et al. also found that simulated LLD changed foot loading patterns and gait-cycle timing, including increased total loading, forefoot loading, hallux loading and changes in propulsion timing (O’Toole et al., 2003).
This is very relevant for podiatry. A small LLD can behave like a pressure-distribution problem. It may influence heel pain, forefoot pain, callus formation, tendon overload, knee symptoms, hip symptoms, or back symptoms, depending on the patient.
3. Knee and hip joint loading
Large cohort studies have linked leg length inequality with osteoarthritis risk, particularly in the shorter limb.
Harvey et al. studied more than 3,000 adults aged 50–79 years and found that radiographic LLD was associated with prevalent, incident symptomatic and progressive knee osteoarthritis. Their study used full-limb radiography and concluded that LLD may be a potentially modifiable risk factor for knee osteoarthritis (Harvey et al., 2010).
Kim et al. examined LLD and hip osteoarthritis using data from the Multicenter Osteoarthritis Study and the Osteoarthritis Initiative. They found that shorter limbs, especially with LLD of at least 2 cm, had increased risk of hip osteoarthritis (Kim et al., 2018).
These studies do not prove that every 5 mm discrepancy causes arthritis. But they support the broader mechanical principle: asymmetrical limb length can alter joint loading over time.
The clinically important “small discrepancy” zone: 5–10 mm
A practical way to think about LLD is to divide it into clinical zones.
- 0–3 mm | Often within measurement error or minor natural asymmetry. Usually not treated unless the clinical pattern is very clear.
- 3–5 mm | Borderline zone. May matter in sensitive patients, runners, dancers, athletes, or people with persistent one-sided symptoms.
- 5–10 mm | Clinically important test zone. Evidence supports that this range can matter, especially in people with standing jobs, chronic low back pain or repeated overuse symptoms.
- 10–20 mm | More clearly biomechanically relevant. Often worth correcting if symptoms or asymmetry are present.
- >20 mm | More likely to require imaging, orthopedic input, shoe build-up, or surgical discussion depending on age, cause and symptoms.
The 5–10 mm group deserves special attention because these patients are often told that nothing is wrong, yet this is the range where conservative care is usually easiest. A small heel lift, custom insole modification, shoe adjustment, or staged correction may be enough to change symptoms.
Defrin et al. specifically studied conservative correction of LLDs of 10 mm or less in patients with chronic low back pain. The study reported that shoe inserts reduced pain and disability in selected patients (Defrin et al., 2005).
Symptoms that may be associated with leg length discrepancy
LLD can produce different symptoms in different people. Some patients are completely asymptomatic. Others develop symptoms after a change in training load, footwear, work demands, ageing, injury, pregnancy, surgery, or weight gain.
Possible symptoms include:
- One-sided low back pain
- Sacroiliac joint discomfort
- Hip pain or hip tightness
- Knee pain, especially on one side
- Heel pain or plantar fasciitis-type symptoms
- Achilles tendon overload
- Forefoot pain or callus under one foot
- Recurrent calf tightness
- Uneven shoe wear
- Feeling “crooked” when standing
- One leg feeling harder to load during running or squatting
- Pelvic drop or trunk lean when walking
- Recurrent overuse injuries on the same side
The pattern matters. LLD should be suspected more strongly when symptoms are recurrent, one-sided, load-related, and associated with measurable asymmetry.
How is leg length discrepancy assessed?
A proper assessment should not rely on one quick test alone. It should combine clinical measurement, posture assessment, gait assessment, footwear review and symptom history.
1. History
This should be detailed and revolve around signs and symptoms frequently associated with leg length inequality.
2. Standing block test
The block test involves placing measured blocks under the shorter side until the pelvis appears level or symptoms improve. Alfuth et al.’s systematic review concluded that the block test appears to be the most useful clinical assessment for LLD, while full-length standing radiography is the stronger imaging reference for anatomical discrepancy (Alfuth et al., 2021).
3. Gait analysis
Gait analysis helps determine whether the discrepancy is functionally relevant. The clinician should observe pelvic drop, trunk lean, step length, foot progression angle, pronation or supination, heel contact, propulsion and asymmetrical loading.
Systematic reviews have shown that LLD can affect stability, kinematics and kinetics during gait (Khamis and Carmeli, 2017; Azizan et al., 2018).
4. Foot pressure analysis
Pressure mapping can be especially useful when symptoms are in the foot, ankle, knee or forefoot. It can show whether one side is overloaded, whether the short side takes higher pressure, whether the long side spends more time in stance, or whether propulsion is asymmetrical.
Pereiro-Buceta et al. demonstrated that simulated LLD changed mean pressure, peak pressure and stance time during gait, supporting the use of dynamic pressure assessment when evaluating loading asymmetry (Pereiro-Buceta et al., 2021).
5. X-rays
Imaging is important when:
- There is a need to distinguish between real and functional LLD
- There is a history of fracture, surgery or growth disorder
- The patient is a child with progressive asymmetry
- There is possibly scoliosis, hip disease, knee arthritis or complex deformity
- Surgery is being considered
Full-length standing radiography is often regarded as a strong reference method for anatomical LLD, but clinical assessment remains important because anatomical length and functional loading are not always the same thing (Alfuth et al., 2021; Sabharwal and Kumar, 2008).
As a clinician managing LLD's for over 20 years, I have often come across patients wearing a heel raise on the wrong leg because a clinician diagnosed a LLD without confirming with x-rays and other suitable tests.
As a clinician managing LLD's for over 20 years, I have often come across patients wearing a heel raise on the wrong leg because a clinician diagnosed a LLD without confirming with x-rays and other suitable tests.
Treatment: should the full discrepancy always be corrected?
Not always.
In some patients, full correction feels immediately better. In others, full correction feels too much because the body has adapted to the discrepancy for years. A staged approach may be safer.
For example, a patient with a 10 mm discrepancy may initially tolerate a 4–6 mm lift better than a full 10 mm correction. Another patient may feel best with 70% correction. Rannisto et al.’s randomized trial corrected 70% of the measured LLD using insoles in workers with standing jobs and low back pain (Rannisto et al., 2019).
The correct amount depends on:
- the size of the discrepancy
- whether it is structural, functional or mixed
- symptoms
- occupation
- sport demands
- footwear
- pelvic and spinal compensation
- patient comfort
- gait response
- pressure response
- adaptation time
This is why self-prescribing a heel lift without assessment can be unreliable. Too little correction may do nothing. Too much correction may irritate the back, hip, knee, Achilles tendon or forefoot.
Can heel lifts or custom insoles help?
Yes, in selected patients.
A heel lift can compensate for a shorter limb by raising the heel or entire foot on that side. A custom insole can do more: it can combine lift correction with arch support, rearfoot control, forefoot accommodation, pressure redistribution and shoe-specific fitting.
Campbell et al. reviewed shoe lifts for adults with painful musculoskeletal conditions associated with LLD. The evidence quality was low, but the available studies generally suggested improvement in pain and function, while also highlighting the need for better trials (Campbell et al., 2018).
D’Amico et al. reported positive short- and long-term effects of customized heel-lift orthotics in patients with nonspecific low back pain and LLD, including reduced pain and improved postural parameters (D’Amico et al., 2022).
The practical conclusion is:
Heel lifts and custom insoles can help when the LLD is clinically relevant, properly measured, corrected gradually if needed, and integrated into the patient’s footwear and gait pattern.
When custom insoles are better than a simple heel lift
A simple heel lift may be enough when the patient has a straightforward structural short leg and no major foot mechanics problem.
Custom insoles may be better when LLD is combined with:
- flat feet
- excessive pronation
- supination
- forefoot overload
- plantar fasciitis
- Achilles tendon pain
- bunions
- knee pain
- hip pain
- diabetic foot pressure risk
- running-related asymmetry
- poor shoe fit
- recurrent callus
- unstable gait
For example, a patient may have a 6 mm shorter right leg, but also excessive pronation on the left foot and forefoot overload on the right. A simple lift may address only one part of the problem. A custom orthotic prescription can address height, alignment and loading together.
Can exercise fix a leg length discrepancy?
It depends on the type of discrepancy.
Exercise cannot lengthen a structurally shorter femur or tibia. If the discrepancy is anatomical, strengthening exercises alone will not make the bones equal.
However, exercise can help when the discrepancy is functional or partly functional. It may improve pelvic control, hip mobility, glute strength, calf flexibility, trunk stability, gait control and load tolerance. In some patients, exercise reduces the symptoms caused by compensation even if the structural difference remains.
The best approach is often combined care:
lift or insole correction for the mechanical height difference, plus exercises to improve the body’s ability to control the correction.
This is especially important because a body that has adapted to asymmetry may need time to adjust. D’Amico et al. noted that LLD equalization requires an adaptation period that varies between individuals (D’Amico et al., 2022).
Frequently asked questions
1. How much of a leg length difference is a problem?
There is no single number that applies to everyone.
A discrepancy of less than 5 mm is often minor, but it may still matter in highly sensitive patients or high-load athletes. A discrepancy of 5–10 mm should not be dismissed if the patient has one-sided symptoms, standing-related pain, recurrent injury, pelvic asymmetry or abnormal gait loading. A discrepancy of 10 mm or more is more likely to be clinically relevant, especially if symptoms match.
Research supports this more nuanced approach. Defrin et al. found that correcting discrepancies of 10 mm or less helped selected patients with chronic low back pain. Rannisto et al. studied correction in standing workers with LLD of at least 5 mm and low back pain, finding clinically important improvements after correction (Defrin et al., 2005; Rannisto et al., 2019).
So the better answer is:
A leg length difference becomes a problem when it creates symptoms, asymmetrical loading, gait compensation or recurrent overuse — and that can happen even below 1 cm.
2. Can exercise fix a leg length difference?
Exercise can help, but it depends on the cause.
If the discrepancy is structural, exercise cannot make the shorter bone longer. But it can improve pelvic stability, hip strength, balance and gait control.
If the discrepancy is functional, exercise may reduce or even resolve the apparent difference by improving posture, joint mobility, muscle balance and movement control.
In many real cases, the best treatment is not “lift or exercise”. It is lift plus exercise, especially when the patient has chronic compensation.
3. Can heel lifts or custom insoles help?
Yes, when prescribed correctly.
Heel lifts can help compensate for a shorter leg. Custom insoles can do more by combining lift correction with control of pronation, supination, arch function, forefoot pressure and shoe fit. The evidence is not perfect, but systematic reviews and clinical studies support the use of shoe lifts in selected patients with LLD-associated musculoskeletal pain (Campbell et al., 2018; Rannisto et al., 2019; D’Amico et al., 2022).
The key is proper assessment. The lift should match the patient’s symptoms, gait, footwear and tolerance. Some patients need gradual correction rather than full correction immediately.
4. Should I go to a polyclinic, podiatrist, orthopedic surgeon, chiropractor or physiotherapist?
The best choice does not depend on the profession but instead depends on whether the clinician is trained and has experience with leg length discrepancies.
A polyclinic or general practitioner is a good starting point if you are unsure what is causing the pain, if there are medical red flags, if imaging may be needed, or if you require referral into the public healthcare system.
A podiatrist is often the most appropriate clinician when the symptoms involve the foot, ankle, heel, forefoot, gait, shoe wear, orthotics or pressure loading. In Singapore, podiatry is recognised within the allied health ecosystem, and podiatrists manage lower-limb and foot-related biomechanical problems, including gait and orthotic management. Note that not all podiatrists are trained or have experience treating LLD's.
A physiotherapist is very useful when the main issue is muscle weakness, hip control, pelvic stability, back pain, rehabilitation, movement retraining or exercise progression. Physiotherapy is particularly valuable when the discrepancy is functional or when the body needs to adapt to a lift. Note that not all physiotherapists are trained or have experience treating LLD's.
An orthopedic surgeon is appropriate when the discrepancy is large, progressive, related to fracture or surgery, associated with significant hip/knee disease, present in a growing child, or when surgical options may need discussion. Note that not all orthopedic surgeons are trained or have experience treating LLD's.
A chiropractor may help some patients with spinal or pelvic symptoms, but if the issue is a true leg length discrepancy, treatment should include objective measurement and a clear plan for lift correction, footwear, gait and loading. Manipulation alone is unlikely to correct an anatomical short leg. Note that not all orthopedic surgeons are trained or have experience treating LLD's.
For many patients, the best pathway is collaborative: podiatry for measurement, gait and orthotic/lift prescription; physiotherapy for strength and control; medical or orthopedic review when surgical opinion is needed.
How Family Podiatry Centre assesses leg length discrepancy
At Family Podiatry Centre, leg length discrepancy is not treated as a number in isolation. It is assessed as part of the patient’s full lower-limb function.
A typical assessment may include:
- symptom history
- standing posture assessment
- pelvic level assessment
- block testing
- foot posture assessment
- footwear review
- walking and/or running gait analysis
- pressure-mapping and force - time curve studies
- assessment of pronation, supination and propulsion
- trial lift testing if needed
- custom insole or heel lift prescription if indicated
- follow-up adjustment after adaptation
The aim is not simply to “make the legs equal”. The aim is to improve comfort, mobility, pressure distribution, gait symmetry and long-term load tolerance.
Key take-home message
Leg length discrepancy should not be dismissed simply because it is less than 1 cm.
A small difference may be harmless in one person and clinically important in another. The difference depends on symptoms, occupation, sport, gait pattern, pelvic compensation, foot pressure, footwear and adaptation.
The most practical clinical message is:
Small leg length discrepancies, especially in the 5–10 mm range, deserve proper assessment when symptoms are present. These discrepancies are often the easiest to treat conservatively, using carefully prescribed heel lifts, custom insoles, footwear modification and rehabilitation exercises.
Disclaimer: The word "treatment" in this article refers to the care and management of a patient’s health to prevent, cure, or improve a condition. Treatment results vary and do not necessarily indicate a cure. This article is for informational and educational purposes only and does not constitute medical advice.
About the author
Mark Reyneker is a podiatrist and human gait specialist with 8 years of training and over 25 years of clinical experience. He is the Founder and Clinical Director of Family Podiatry Centre and has a Bachelors degree in Podiatric Medicine and a Master’s degree in paleoanthropology, with research focused on human foot function and metatarsal loading.
Social Media Link
Disclaimer: The word "treatment" in this article refers to the care and management of a patient’s health to prevent, cure, or improve a condition. Treatment results vary and do not necessarily indicate a cure. This article is for informational and educational purposes only and does not constitute medical advice.
About the author
Mark Reyneker is a podiatrist and human gait specialist with 8 years of training and over 25 years of clinical experience. He is the Founder and Clinical Director of Family Podiatry Centre and has a Bachelors degree in Podiatric Medicine and a Master’s degree in paleoanthropology, with research focused on human foot function and metatarsal loading.
Social Media Link
References
10. O’Toole, G.C., Makwana, N.K., Lunn, J., Harty, J. and Stephens, M.M. (2003) ‘The effect of leg length discrepancy on foot loading patterns and contact times’, Foot & Ankle International, 24(3), pp. 256–259.
11. Pereiro-Buceta, H., Becerro-de-Bengoa-Vallejo, R., Losa-Iglesias, M.E., López-López, D., Navarro-Flores, E., Martínez-Jiménez, E.M., Martiniano, J. and Calvo-Lobo, C. (2021) ‘The effect of simulated leg-length discrepancy on the dynamic parameters of the feet during gait—cross-sectional research’, Healthcare, 9(8), 932.