Leg Length Differences After Hip or Knee Surgery
8 June 2026
By By Mark Reyneker, B.T. Pod (SA), MSc (SA) Registered Podiatrist & Human Gait Specialist Founder | Clinical Director, Family Podiatry Centre

Published: 8 June 2026 | Last reviewed: 8 June 2026
Leg length discrepancy (LLD) after hip or knee surgery is not rare, but it is often misunderstood. The important distinction is between radiographic LLD, functional LLD, and perceived LLD. A patient may feel uneven even when X-rays show only a small difference, and another patient may tolerate a measurable discrepancy quite well. This is why treatment should be based on the patient’s symptoms, gait, pelvic position, footwear, and objective measurement, not on X-ray numbers alone.
1. What is LLD after surgery?
After hip or knee surgery, LLD may be:
Anatomical / structural LLD
A true difference in skeletal limb length, often measurable on long-leg standing radiographs.
A true difference in skeletal limb length, often measurable on long-leg standing radiographs.
Functional / apparent LLD
The limbs may be similar in bony length, but pelvic obliquity, hip contracture, knee flexion contracture, foot pronation/supination, scoliosis, abductor weakness, or altered gait makes one limb behave as though it is shorter.
The limbs may be similar in bony length, but pelvic obliquity, hip contracture, knee flexion contracture, foot pronation/supination, scoliosis, abductor weakness, or altered gait makes one limb behave as though it is shorter.
Perceived LLD
The patient feels uneven, even when measured LLD is small or absent. This is especially common after hip replacement and can strongly affect satisfaction and confidence.
The patient feels uneven, even when measured LLD is small or absent. This is especially common after hip replacement and can strongly affect satisfaction and confidence.
A 2021 systematic review concluded that the block test is probably the most useful clinical assessment, while full-length standing anteroposterior radiography is the most valid reference method for anatomical LLD (Alfuth, Fichter and Knicker, 2021).
2. How common is LLD after hip replacement?
LLD is a well-recognised complication after total hip arthroplasty (THA). A recent review reported that LLD after THA occurs in approximately 3% to 30% of cases, with mean discrepancies commonly reported between 3 and 17 mm (Bianco Prevot et al., 2025). The same review notes that LLD after THA may be associated with gait disturbance, back pain, postural imbalance, dissatisfaction, and medico-legal concerns.
Older but influential THA literature shows why the issue matters. Konyves and Bannister (2005) found that postoperative leg lengthening was common and that perceived length discrepancy could persist at 12 months. Wylde et al. (2009) found that 30% of hip replacement patients reported perceived LLD, and those patients had poorer Oxford Hip Scores and more limping than those who did not perceive LLD.
In THA, the surgeon has to balance several priorities:
- restoring hip stability;
- restoring femoral offset;
- correcting pre-existing deformity or contracture;
- preventing dislocation;
- restoring leg length where possible.
Sometimes a slightly longer limb is accepted intra-operatively because a stable hip is safer than a perfectly equal but unstable hip. However, even small changes can feel large to the patient, especially if they already had pelvic compensation before surgery.
3. How common is LLD after knee replacement?
LLD after total knee arthroplasty (TKA) is less discussed than after THA, but it is clinically important. TKA can lengthen the operated limb because correction of varus, valgus, or flexion deformity straightens the limb mechanically. A systematic review and meta-analysis found average limb lengthening of about 5.98 mm after TKA, with reported postoperative LLD ranging widely; radiographic postoperative LLD was reported in 44% to 83.3% of patients across included studies (Tripathy et al., 2021).
A prospective cohort study found that radiographic LLD of 10 mm or more after TKA significantly worsened functional outcome. In that study, 91.1% of patients had some limb lengthening after TKA, and perceived LLD decreased from 34.5% preoperatively to 3.7% postoperatively (Pradhan et al., 2022).
The common mechanism is not that the surgeon “adds length” in the same way as THA. Rather, the knee is often surgically corrected from a deformed position into a straighter mechanical axis. A varus knee, valgus knee, or flexed knee may functionally shorten the limb before surgery. When alignment improves, the limb may become mechanically longer.
This is especially relevant in patients who have:
- severe varus deformity;
- severe valgus deformity;
- fixed flexion deformity;
- unilateral knee replacement when both knees are arthritic;
- delayed replacement after years of compensation.
4. How LLD affects the patient
LLD can affect the patient mechanically, neurologically, emotionally, and behaviourally.
Gait and balance
A short limb may cause pelvic drop, early heel rise, increased knee flexion, circumduction, hip hiking, or asymmetric stride length. A long limb may cause vaulting, reduced knee flexion clearance, or a feeling of “jamming” into the hip, knee, or lower back.
A short limb may cause pelvic drop, early heel rise, increased knee flexion, circumduction, hip hiking, or asymmetric stride length. A long limb may cause vaulting, reduced knee flexion clearance, or a feeling of “jamming” into the hip, knee, or lower back.
Pelvic and spinal compensation
Even small LLD can create pelvic obliquity. Over time, the patient may develop compensatory lumbar side-bending, altered sacroiliac loading, or increased paraspinal muscle activity. D’Amico, Kinel and Roncoletta (2022) describe associations between LLD, altered spinopelvic alignment, postural change, low back pain, and altered underfoot loading.
Even small LLD can create pelvic obliquity. Over time, the patient may develop compensatory lumbar side-bending, altered sacroiliac loading, or increased paraspinal muscle activity. D’Amico, Kinel and Roncoletta (2022) describe associations between LLD, altered spinopelvic alignment, postural change, low back pain, and altered underfoot loading.
Pain
Common symptom patterns include:
Common symptom patterns include:
- low back pain;
- hip pain or groin discomfort;
- lateral hip irritation;
- knee discomfort;
- foot and ankle overload;
- calf fatigue;
- recurrent “one-sided” muscle tightness;
- difficulty standing for long periods.
Patient confidence and satisfaction
This is particularly important after surgery. A patient may have technically successful hip or knee replacement but still feel that “something is wrong” because the ground no longer feels level. THA studies repeatedly associate perceived LLD with dissatisfaction, poorer function, and limping (Wylde et al., 2009; Röder et al., 2012).
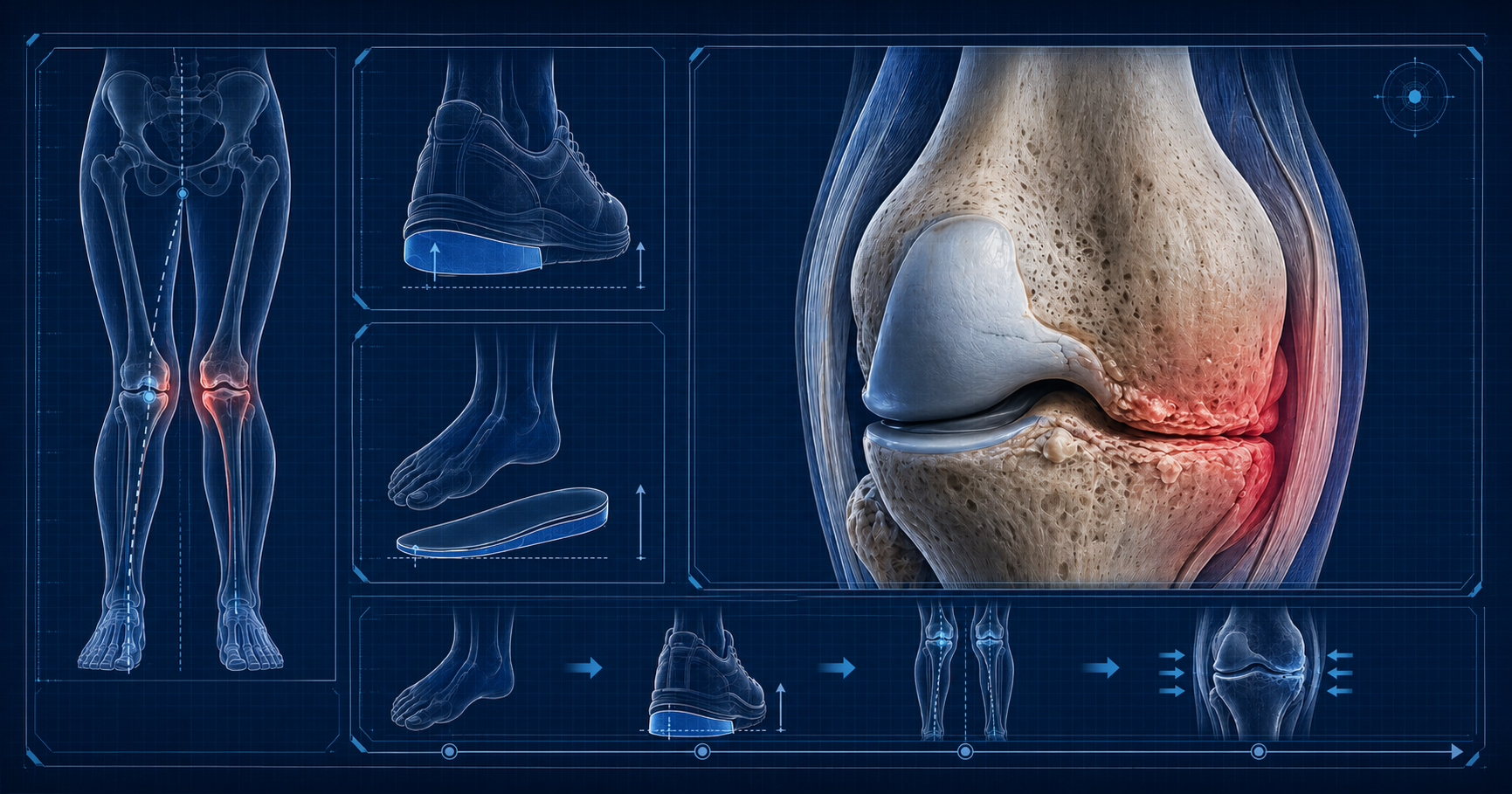
5. Why heel raises, lifts, and orthotics can help
The conservative logic is straightforward: if one side is functionally or structurally short, a lift can reduce pelvic obliquity and improve the timing of gait.
D’Amico, Kinel and Roncoletta (2022) studied 80 patients with nonspecific low back pain and LLD using customized orthotics with 100% LLD heel-lift correction. Pain scores improved from an average of 7.8 initially to 1.1 at four months and 0 at two years, with improvements in frontal-plane postural parameters and no worsening reported.
However, this does not mean every post-surgical patient should automatically receive full correction immediately. Postoperative patients may have soft-tissue adaptation, swelling, abductor weakness, knee stiffness, or pelvic compensation that changes during rehabilitation. A careful trial is usually better than guessing.
6. Heel raise versus full-length lift versus custom orthotic
Simple heel raise
A simple heel raise can be useful when:
- the discrepancy is small;
- the patient needs a quick trial;
- there is enough shoe depth;
- symptoms are mainly pelvic/back/hip related;
- the foot is otherwise mechanically stable.
It is usually the simplest way to test whether raising the short side improves symptoms.
Full-length lift
A full-length lift is often better when:
- the correction is more than a few millimetres;
- the patient feels forefoot imbalance;
- the heel lift pushes the foot forward in the shoe;
- the patient develops calf tightness;
- there is forefoot overload;
- the patient needs a more natural rollover.
A full-length lift avoids concentrating the correction only under the heel. D’Amico et al. used customized orthotics with the lift shaped from the calcaneus to the Lisfranc joint, which is closer to a controlled full-foot correction than a loose heel wedge.
Custom orthotic / insole with lift
A custom orthotic is preferable when LLD exists alongside:
- excessive pronation;
- excessive supination;
- unstable midfoot mechanics;
- knee valgus or varus compensation;
- plantar fasciitis;
- metatarsalgia;
- post-THA Trendelenburg-type gait;
- altered pressure under one forefoot;
- different left/right foot mechanics.
This matters because many post-surgical patients do not only have a “length problem”. They often also have a loading problem.
7. Suggested clinical pathway
Step 1: Rule out surgical complications
A new or worsening LLD sensation after THA or TKA should first be reviewed by the surgeon, especially if there is severe pain, instability, sudden change, suspected dislocation, fracture, implant issue, infection, or neurological symptoms.
Step 2: Measure clinically
Use:
- standing posture assessment;
- iliac crest / ASIS / PSIS comparison;
- block test under the shorter side;
- gait observation;
- footwear inspection;
- treadmill or pressure analysis where available.
The block test is clinically useful because it assesses the patient in weight-bearing and captures some functional components of LLD (Alfuth, Fichter and Knicker, 2021).
Step 3: Decide whether the problem is structural, functional, perceived, or mixed
This is the critical podiatric step. A patient may have a 6 mm structural difference but a 12 mm functional pelvic compensation. Another may have a measurable 10 mm difference but no symptoms. Treatment should match the patient, not only the ruler.
Step 4: Trial a temporary lift
A practical approach is to start with a temporary lift and review the response. Improvement in standing comfort, gait symmetry, back pain, hip comfort, or confidence is clinically meaningful.
Step 5: Convert to a definitive device
If the trial helps, then convert to:
- heel raise;
- full-length lift;
- custom orthotic with lift;
- external shoe raise if the amount is too large to fit inside the shoe.
Step 6: Reassess after adaptation
Patients often need time to adapt. Recheck gait, pelvis, symptoms, footwear, and pressure distribution. Overcorrection can be as problematic as undercorrection.
8. Important nuance: small discrepancies can matter
Traditional orthopaedic teaching often implies that small LLD is harmless. That is too simplistic. The evidence is mixed, but multiple studies show that symptoms depend on more than the number of millimetres. Patient perception, pelvic mobility, spinal compensation, foot mechanics, abductor strength, and the timing of postoperative rehabilitation all influence whether a discrepancy becomes symptomatic.
This is especially relevant after hip and knee surgery because the patient’s nervous system has adapted to years of arthritis, deformity, pain avoidance, and asymmetrical gait. Surgery changes the mechanical environment quickly, but neuromuscular adaptation can take much longer.
9. Clinical conclusion
LLD after hip and knee surgery is common enough to be actively assessed, especially when a patient reports limping, back pain, hip discomfort, knee discomfort, imbalance, or “one leg feels longer”. After THA, LLD is widely reported and can affect satisfaction. After TKA, limb lengthening is common because deformity correction changes the mechanical limb axis; LLD of 10 mm or more appears more likely to affect functional outcome.
Heel raises, full-length lifts, and orthotic insoles are not just “padding”. Used properly, they are mechanical interventions that can reduce pelvic obliquity, improve gait symmetry, reduce compensatory loading, and restore confidence. The best results come from measuring, trialling, observing gait, and individualising the correction.
If you feel uneven after hip or knee surgery, or if you have developed limping, back pain, hip discomfort, or foot pain, a podiatric gait assessment can help determine whether a heel raise, shoe lift, or custom orthotic insole may improve your walking comfort.
Book An Appointment
Disclaimer: The word "treatment" in this article refers to the care and management of a patient’s health to prevent, cure, or improve a condition. Treatment results vary and do not necessarily indicate a cure. This article is for informational and educational purposes only and does not constitute medical advice.
About the author
Mark Reyneker is a podiatrist and human gait specialist with 8 years of training and over 25 years of clinical experience. He is the Founder and Clinical Director of Family Podiatry Centre and has a Bachelors degree in Podiatric Medicine and a Master’s degree in paleoanthropology, with research focused on human foot function and metatarsal loading.
If you feel uneven after hip or knee surgery, or if you have developed limping, back pain, hip discomfort, or foot pain, a podiatric gait assessment can help determine whether a heel raise, shoe lift, or custom orthotic insole may improve your walking comfort.
Book An Appointment
Disclaimer: The word "treatment" in this article refers to the care and management of a patient’s health to prevent, cure, or improve a condition. Treatment results vary and do not necessarily indicate a cure. This article is for informational and educational purposes only and does not constitute medical advice.
About the author
Mark Reyneker is a podiatrist and human gait specialist with 8 years of training and over 25 years of clinical experience. He is the Founder and Clinical Director of Family Podiatry Centre and has a Bachelors degree in Podiatric Medicine and a Master’s degree in paleoanthropology, with research focused on human foot function and metatarsal loading.
References
6. Desai, A.S., Dramis, A. and Board, T.N. (2013) ‘Leg length discrepancy after total hip arthroplasty: A review of literature’, Current Reviews in Musculoskeletal Medicine, 6, pp. 336–341. doi:10.1007/s12178-013-9180-0.
7. Goldstein, Z.H., Yi, P.H., Batko, B., Kearns, S., Tetreault, M.W., Levine, B.R., Della Valle, C.J. and Sporer, S.M. (2016) ‘Perceived leg-length discrepancy after primary total knee arthroplasty: Does knee alignment play a role?’, American Journal of Orthopedics, 45, pp. E429–E433.
8. Hinarejos, P., Sánchez-Soler, J., Leal-Blanquet, J., Torres-Claramunt, R. and Monllau, J.C. (2020) ‘Limb length discrepancy after total knee arthroplasty may contribute to suboptimal functional results’, European Journal of Orthopaedic Surgery & Traumatology, 30, pp. 1199–1204. doi:10.1007/s00590-020-02683-6.
9. Konyves, A. and Bannister, G.C. (2005) ‘The importance of leg length discrepancy after total hip arthroplasty’, The Journal of Bone and Joint Surgery. British Volume, 87-B(2), pp. 155–157. doi:10.1302/0301-620X.87B2.14878.
10. Lang, J.E., Scott, R.D., Lonner, J.H., Bono, J.V., Hunter, D.J. and Li, L. (2012) ‘Magnitude of limb lengthening after primary total knee arthroplasty’, The Journal of Arthroplasty, 27, pp. 341–346. doi:10.1016/j.arth.2011.06.008.
11. Pradhan, S.S., Tripathy, S.K., Jain, M., Behera, H., Velagada, S. and Srinivasan, A. (2022) ‘Impact of limb length discrepancy on functional outcome in total knee arthroplasty patients: A prospective cohort study’, Arthroplasty, 4, 22. doi:10.1186/s42836-022-00123-w.
12. Röder, C., Vogel, R., Burri, L., Dietrich, D. and Staub, L.P. (2012) ‘Total hip arthroplasty: Leg length inequality impairs functional outcomes and patient satisfaction’, BMC Musculoskeletal Disorders, 13, 95. doi:10.1186/1471-2474-13-95.
13. Sabir, A.B., Faizan, M., Ishtiaq, M., Jilani, L.Z., Ahmed, S. and Shaan, Z.H. (2020) ‘Limb length discrepancy after total knee arthroplasty: Unilateral versus bilateral, a comparative study at tertiary centre’, Journal of Clinical Orthopaedics and Trauma, 11(Suppl 5), pp. S740–S745. doi:10.1016/j.jcot.2020.06.041.
14. Tripathy, S.K., Pradhan, S.S., Varghese, P., Purudappa, P.P., Velagada, S., Goyal, T., Panda, B.B. and Vanyambadi, J. (2021) ‘Limb length discrepancy after total knee arthroplasty: A systematic review and meta-analysis’, World Journal of Clinical Cases, 9(2), pp. 357–371. doi:10.12998/wjcc.v9.i2.357.
15. Vaidya, S.V., Patel, M.R., Panghate, A.N. and Rathod, P.A. (2010) ‘Total knee arthroplasty: Limb length discrepancy and functional outcome’, Indian Journal of Orthopaedics, 44, pp. 300–307. doi:10.4103/0019-5413.65159.