Flat Feet Are Not Always Permanent
18 May 2026
For many years, patients with flat feet have often been told the same thing: “You cannot change the shape of the foot. Orthotics only help with pain or are designed to make you more comfortable”. This statement is repeated frequently in clinics, insurance discussions and, more recently, on social media. It sounds plausible, especially when said by a clinician, but it is often based on a rudimentary understanding of foot function and biomechanics.
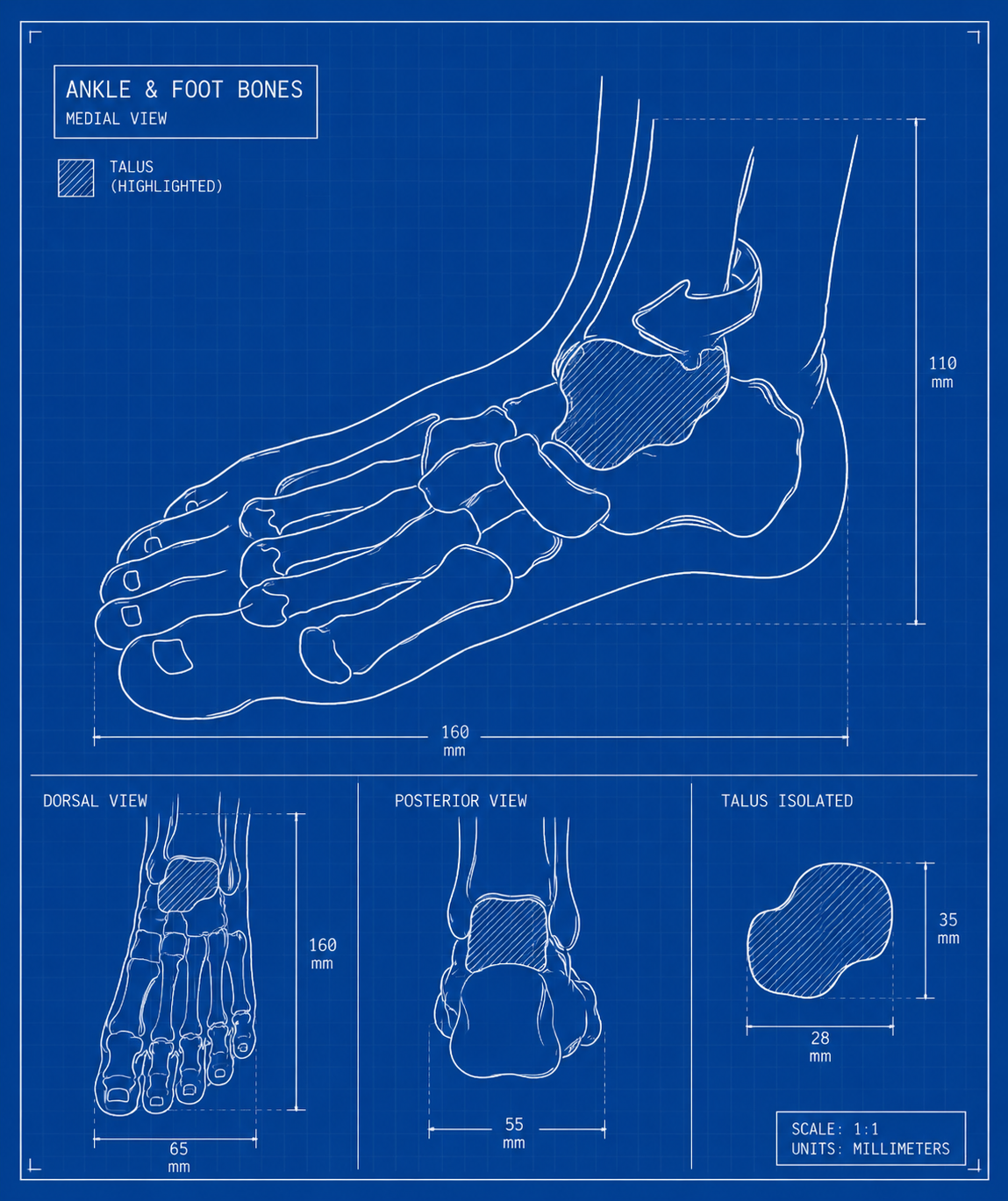
At Family Podiatry Centre, our clinical experience and years of biomechanics training, has led us to a different conclusion. Many flexible flat feet are not simply “low arches”. They are often feet in which the talus — the central bone sitting between the leg and the foot — is excessively plantarflexed, adducted (pointing down towards the ground) or mal-aligned under body weight. When this talar position improves, the arch improves with it.
This does not mean that every flat foot can be “cured”, nor that every person with flat feet needs treatment. It does mean that the common statement “flat feet cannot be corrected or improved” is incorrect and misleading.
The problem with the old flat foot classification
Traditional flat foot classification usually begins with a simple division:
- Flexible flat foot — the arch appears when the foot is not bearing weight or when the patient stands on tiptoe.
- Rigid flat foot — the arch remains collapsed even when non-weight-bearing.
This classification is useful as a starting point, but it is not enough to guide treatment. It tells us whether the foot is flexible or rigid, but it does not tell us why the foot collapses, which structure is driving the deformity, how reducible the deformity is, or where an orthotic should apply corrective force.
Recent literature acknowledges this problem. Kim et al. note that flatfoot is commonly classified into flexible and rigid types, but also state that there is no consensus on clinical or radiographic definitions of flatfoot. Their study used radiographic measurements to assess changes after long-term insole treatment, which is exactly the type of objective approach needed if we are to move beyond visual labels alone (Kim et al., 2023).
The “flexible versus rigid” model is therefore descriptive, not prescriptive. It describes what the foot looks like under certain conditions. It does not adequately explain the mechanics of correction. Clinicians who stick to this simplistic classification will be misled into simplistic treatment options for the patient. Options such as "its rigid so it cannot be treated" or "it's flexible so wear insoles for comfort for the rest of your life".
Why the talus matters
The talus is not just another bone in the foot. It is the mechanical link between the leg and the rest of the foot. It sits under the tibia and fibula, forms part of the ankle joint, and articulates with the calcaneus and navicular. Unlike many other bones, it has no direct muscular attachment. Its position is therefore controlled indirectly by joint alignment, ligament tension, body weight, muscle function and external devices such as orthotics.
Seringe and Wicart described the talonavicular and subtalar joints as part of a linked subtalar joint complex. Their “calcaneopedal unit” concept separates the talus, which is held by the ankle mortise, from the rest of the foot, which moves around it. This model helps explain why talar malalignment can create a planovalgus foot posture (flat feet) and why treating the arch alone may miss the true driver of the deformity (Seringe and Wicart, 2013).
In a flexible flat foot, the apparent arch collapse is often the visible consequence of a deeper three-dimensional positional problem. The talus may sit too low and too medially under load. The navicular follows the talar head. The medial column lowers. The heel drifts into valgus. The forefoot may abduct. To the untrained eye, this looks like “a low arch”. To the clinician who understands talar mechanics, it is more accurately a talus-led collapse of the foot structure.
Talar declination angle: a more meaningful measurement
One of the most useful measurements in this context is the talar declination angle. This is measured on a weight-bearing lateral foot X-ray. It shows how steeply the talus is angled downward toward the supporting surface.
In many flexible flat feet, the talar declination angle is increased. This means the talus is excessively plantarflexed under load. When the talus sits too low, the medial longitudinal arch also appears lower. Therefore, instead of merely asking, “Is the arch flat?”, a better question is:
Is the talus excessively declined, and can this position be improved?
Is the talus excessively declined, and can this position be improved?
This shift in thinking is important. It changes flat foot management from “supporting an arch” to reducing a talar malalignment.
A talus-centred approach therefore uses the weight-bearing lateral X-ray not as a passive diagnostic image, but as a treatment map. The clinician can measure the talar declination angle, prescribe an orthotic intended to improve the talar position, and then reassess the radiographic change over time.
Orthotics should not simply prop up the arch
One of the most common mistakes in flat foot treatment is assuming that the arch is the primary target. Many over-the-counter insoles are designed around this assumption. They place a soft bump under the medial arch and are marketed as “arch supports”.
The problem is that the arch is often not the driver of the deformity. The arch is the result of the deformity. If the talus remains excessively declined and medially displaced, a soft arch pad may simply compress, deform or push into the wrong area. It may give temporary comfort, but it is unlikely to produce meaningful mechanical change.
Ahn et al. studied talus control foot orthoses in children with flexible flatfoot. These orthoses were designed with an upright portion rising above the navicular to cover and protect the talonavicular joint. The authors reported that both rigid foot orthoses and talus control foot orthoses improved clinical and radiographic measurements, but talus control orthoses produced greater improvement in certain measurements, including anteroposterior talocalcaneal angle and resting calcaneal stance position (Ahn et al., 2017).
This is highly relevant. It supports the idea that effective orthotic treatment is not merely about filling the arch. It is about influencing the position and movement of the talus, navicular, calcaneus and medial column under load.
Evidence that orthoses can change radiographic alignment
A major reason some clinicians dismiss orthotic treatment is that they assume orthoses only reduce symptoms. Pain relief is important, but it is not the whole story.
There is peer-reviewed evidence that orthoses can improve radiographic parameters in selected children with flexible flat feet. Kim et al. studied 200 children under 18 years old with symptomatic flexible flatfoot who were treated with periodically revised insoles and followed with weight-bearing lateral radiographs. They found significant improvement in calcaneal pitch angle and talo-first metatarsal angle after treatment. The authors concluded that long-term, periodically revised insoles could reduce symptoms and improve radiologic indices (Kim et al., 2023).
Similarly, Liu et al. published a systematic review and meta-analysis examining radiological parameters and pain in children with flexible flat feet. They found that foot orthoses significantly improved radiological parameters in older children, especially the lateral talar-first metatarsal angle, lateral talo-heel angle and calcaneal pitch angle. The authors concluded that orthoses positively affected radiological parameters and reduced pain in older children with flexible flat feet (Liu et al., 2024).
This evidence does not prove that every flat foot can be permanently corrected. It does, however, directly challenges the claim that orthoses are only palliative devices with no structural influence.
Why some studies appear to show limited benefit
There are studies and reviews that appear cautious about foot orthoses for paediatric flat feet. These papers are important, but they must be interpreted carefully.
The Cochrane review by Evans et al. found that evidence was limited and heterogeneous, and that there was no optimal strategy or consensus for using foot orthoses in paediatric flat feet. However, the review included varied populations, including asymptomatic children, symptomatic children and children with other conditions such as juvenile idiopathic arthritis. It also compared different orthotic designs, footwear approaches and outcome measures (Evans et al., 2022).
This matters because “foot orthoses” are not all the same. A soft prefabricated arch pad, a semi-rigid insole, a custom-moulded device, a UCBL-type orthosis and a talus-control orthosis are mechanically different interventions. If all of these are grouped together, the result may understate the value of a properly prescribed device for a clearly defined mechanical problem.
Oerlemans et al. also highlighted heterogeneity in studies of orthoses for flexible flatfeet in children and adults. Their review found that conclusions were difficult because study designs, populations and outcome measures varied substantially (Oerlemans et al., 2023).
This is not evidence that orthoses do not work. It is evidence that the research question has often been too vague.
A better question is not:
Do orthotics work for flat feet?
Do orthotics work for flat feet?
A better question is:
In which type of flexible flat foot, with which radiographic pattern, at what age, using which orthotic design, with what footwear, over what period of time, and measuredby which structural and functional outcomes?
In which type of flexible flat foot, with which radiographic pattern, at what age, using which orthotic design, with what footwear, over what period of time, and measuredby which structural and functional outcomes?
That is where a talus-centred classification becomes clinically useful.
The Family Podiatry Centre approach: treating the talus, not just the arch
In our clinical approach, the assessment of flexible flat feet does not stop at looking at the arch. We are particularly interested in the position of the talus under body weight.
This gives an objective baseline. Custom orthotics can then be prescribed with the aim of improving the talar position over time.
The process is not instant. It is closer to orthodontics than to simple cushioning. A dentist does not correct crowded teeth by giving the patient a soft mouthguard. The dentist uses a carefully designed appliance to apply controlled forces over time. In the same way, a properly designed custom orthotic is not merely a comfort device. It is a mechanical interface between the foot, the shoe and the ground.
In our experience, when the orthotic is designed around talar reduction rather than simple arch propping, many flexible flat feet can show measurable improvement over time. The change is often seen as improvement in talar declination, improved talo-first metatarsal alignment, improved arch profile and better overall foot posture.
This clinical observation is consistent with the broader direction of the literature: radiographic measurements can improve with orthotic treatment, especially when the device is designed to control the relevant mechanics rather than merely cushion the arch (Ahn et al., 2017; Kim et al., 2023; Liu et al., 2024).
Why ready-made insoles are not equivalent to custom orthotics
Over-the-counter insoles can be useful in some situations. They may provide cushioning, comfort or mild support. However, they should not be presented as equivalent to custom orthotics for a patient whose foot requires specific mechanical correction.
The issue is not simply “custom versus non-custom”. The issue is whether the device is capable of applying the right force, in the right place, with the right stiffness, inside the right shoe, for the right foot type.
A soft insole may feel comfortable, but if it collapses under body weight, it cannot meaningfully influence talar position. If the arch support is placed too far back, too far forward, too low or too medially, it may fail to control the talonavicular region. If the shoe is too flexible or unstable, even a good orthotic may not work properly.
This is why insurance policies and online advice can become problematic when they treat all insoles as interchangeable. A custom orthotic prescribed to influence talar declination and talonavicular mechanics is not the same intervention as a soft retail arch support. Grouping them together is like saying reading glasses, contact lenses and surgical lens implants are all “eye products”, therefore any one of them will do.
The clinical question should not be whether a product is called an “orthotic”. The question should be whether it is mechanically appropriate for the deformity being treated.
Why the “flat feet cannot be improved” message is harmful
Patients with flat feet often arrive after years of being told that nothing can be done. Some are told that their feet are simply genetic. Others are told that orthotics are only for pain. Some are told that unless the foot is painful, it should be ignored entirely.
There is some truth in this. Not every flat foot requires treatment. Many children have flexible flat feet that improve naturally. Some adults have flat feet with no pain or functional limitation. These people may not need orthotics.
But this truth has been stretched too far. It has become a blanket statement that denies help to patients who may benefit from treatment. When patients with reducible flat feet, abnormal talar declination, fatigue, pain, gait problems, shoe-wear problems or progressive collapse are told that nothing can be improved, they may lose the opportunity for early, conservative mechanical correction.
The literature supports a more nuanced position. Hsieh et al. found that children with symptomatic flexible flatfoot who wore customized arch support insoles for 12 weeks showed significant improvement in pain/comfort, physical health, stair ascent time and mobility-related measures compared with controls, although the authors called for larger studies because of baseline group differences (Hsieh et al., 2018).
The correct message to patients should not be “flat feet are always a problem” or “flat feet can never be improved”.
The correct message is:
Some flat feet are harmless. Some are symptomatic. Some are reducible. Some are progressive. Some can improve with the right treatment. The key is proper assessment.
The correct message is:
Some flat feet are harmless. Some are symptomatic. Some are reducible. Some are progressive. Some can improve with the right treatment. The key is proper assessment.
A better classification: talus-centred flat foot assessment
A more useful classification of flexible flat feet should include the talus. Instead of classifying only by arch height or flexibility, clinicians should ask:
- Is the talar declination angle increased?
- Is the talus plantarflexed excessively under load?
- Is there talonavicular uncovering or medial talar head prominence?
- Is the deformity reducible manually or during functional testing?
- Is the heel valgus driven primarily by subtalar compensation?
- Is there forefoot abduction?
- Is there medial column instability?
- Is there equinus contributing to compensation?
- Is the patient still growing, skeletally mature, or somewhere in between?
- Does the foot respond to temporary correction, taping, footwear change or test orthotic loading?
This approach produces a treatment-guiding classification, not just a descriptive label.
A patient with a flexible flat foot and increased talar declination may need a very different orthotic strategy from a patient whose main issue is midfoot collapse, severe ligamentous laxity, forefoot varus, equinus or rigid coalition. A talus-centred assessment does not ignore the rest of the foot. It simply recognises that the talus is often the key structural driver of the deformity.
Orthotic treatment is not passive support
A properly prescribed custom orthotic should not be thought of as a passive insert. It is an active mechanical device. Its role may include:
- improving talar position under load;
- reducing excessive subtalar and midtarsal joint compensation;
- supporting the talonavicular region;
- improving the relationship between the rearfoot and forefoot;
- redistributing plantar pressure;
- improving gait efficiency;
- reducing tissue overload;
- allowing the foot to function in a more mechanically favourable position over time.
This is very different from simply “putting something under the arch”.
The distinction is important because many dismissals of orthotic therapy are based on outdated or poorly specified orthotic concepts. If an orthotic is too soft, poorly fitted, placed in unstable shoes or designed only as a cushion, then it may indeed fail to produce meaningful structural change. But that failure should not be used to dismiss properly prescribed custom orthotics based on radiographic and biomechanical assessment.
Conclusion: flat feet requires a nuanced approach
Flat feet are not all the same. Some are normal developmental variants. Some are painless and require no treatment. Some are rigid and need further investigation. But many flexible flat feet are reducible, measurable and mechanically influenced by the position of the talus.
The talus-centred approach challenges the outdated idea that flat feet are simply low arches. It also challenges the equally simplistic idea that orthotics only reduce symptoms and cannot influence structure.
The scientific literature supports several key points: flatfoot classification remains inconsistent; radiographic parameters can improve with orthotic treatment in selected children; talus-control orthoses can produce better correction than standard rigid orthoses in some measures; and the talonavicular-subtalar complex is central to understanding planovalgus deformity (Seringe and Wicart, 2013; Ahn et al., 2017; Kim et al., 2023; Liu et al., 2024).
Patients should not be given false hope. But they should also not be given false hopelessness.
For the right patient, with the right assessment, the right X-rays, the right orthotic design and the right follow-up, flexible flat feet may be improved. The goal is not merely to cushion pain. The goal is to understand the mechanics of the foot and, where possible, guide it toward a better structural and functional position.
The Family Podiatry Centre has successfully treated/reduced flat feet in patients throughout Singapore and Malaysia using the talus centred approach. The protocol was pioneered in S.E. Asia by podiatrist Mark Reyneker. While hundreds of patients have improved under our care, sadly many have been misled into thinking that the diagnosis of flat feet is permanent and not reducible. It is our hope that many more will seek assistance in managing their flat feet with clinicians that have a broader more nuanced understanding of the consition.
The Family Podiatry Centre has successfully treated/reduced flat feet in patients throughout Singapore and Malaysia using the talus centred approach. The protocol was pioneered in S.E. Asia by podiatrist Mark Reyneker. While hundreds of patients have improved under our care, sadly many have been misled into thinking that the diagnosis of flat feet is permanent and not reducible. It is our hope that many more will seek assistance in managing their flat feet with clinicians that have a broader more nuanced understanding of the consition.
Disclaimer: The word "treatment" in this article refers to the care and management of a patient’s health to prevent, cure, or improve a condition. Treatment results vary and do not necessarily indicate a cure. This article is for informational and educational purposes only and does not constitute medical advice.
References
1. Ahn, S.Y., Bok, S.K., Kim, B.O. and Park, I.S. (2017) ‘The effects of talus control foot orthoses in children with flexible flatfoot’, Journal of the American Podiatric Medical Association, 107(1), pp. 46–53. doi: 10.7547/15-045.
2. Evans, A.M., Rome, K., Carroll, M. and Hawke, F. (2022) ‘Foot orthoses for treating paediatric flat feet’, Cochrane Database of Systematic Reviews, 2022(1), CD006311. doi: 10.1002/14651858.CD006311.pub4.
3. Hsieh, R.L., Peng, H.L. and Lee, W.C. (2018) ‘Short-term effects of customized arch support insoles on symptomatic flexible flatfoot in children: a randomized controlled trial’, Medicine, 97(20), e10655. doi: 10.1097/MD.0000000000010655.
4. Kim, J.Y., Kim, S.A., Kim, Y., Hwang, I. and Heo, N.H. (2023) ‘Radiologic changes of long term foot insole use in symptomatic pediatric flatfoot’, Medicine, 102(10), e33152. doi: 10.1097/MD.0000000000033152.
6. Oerlemans, L.N.T., Peeters, C.M.M., Munnik-Hagewoud, R., Nijholt, I.M., Witlox, A. and Verheyen, C.C.P.M. (2023) ‘Foot orthoses for flexible flatfeet in children and adults: a systematic review and meta-analysis of patient-reported outcomes’, BMC Musculoskeletal Disorders, 24, 16. doi: 10.1186/s12891-022-06044-8.
7. Seringe, R. and Wicart, P. (2013) ‘The talonavicular and subtalar joints: the “calcaneopedal unit” concept’, Orthopaedics & Traumatology: Surgery & Research, 99(6 Suppl), pp. S345–S355. doi: 10.1016/j.otsr.2013.07.003.
Written and prepared by:
Mark Reyneker
Written and prepared by:
Mark Reyneker
B.T. Pod (SA), MSc (SA)
Podiatrist and Human Gait Specialist
Registered with the Podiatry Association of Singapore
Founder and Director:
Family Podiatry Centre Pte Ltd
Family Podiatry Centre Sdn Bhd
Solescape Orthotics Laboratory
Solescape Shoes brand