A Parent’s Guide to Intoeing
1 June 2026
By Mark Reyneker, B.T. Pod (SA), MSc (SA) Registered Podiatrist & Human Gait Specialist | Founder & Clinical Director, Family Podiatry Centre
Published: 1 June 2026 | Last reviewed: 18 June 2026
Intoeing is one of the most common walking concerns parents notice in children. It is often described as “pigeon-toed” walking, where one or both feet turn inward instead of pointing straight ahead. For many children, intoeing is part of normal development and improves as they grow. However, some children trip frequently, look awkward when running, wear shoes unevenly, or become self-conscious about the way they walk. In those cases, careful assessment and sensible nonsurgical treatment can make a meaningful difference.
The key message is this: intoeing is not one diagnosis. It can come from the foot, the shin bone, the thigh bone, or a combination of these. Treatment should therefore be based on where the rotation is coming from, how severe it is, whether the child is symptomatic, and whether the problem is improving or persisting.
1. What is intoeing?
Intoeing means that the feet turn inward during walking or running. The medical term usually used during gait assessment is the foot progression angle. If the foot points inward relative to the direction of walking, the foot progression angle is described as internally rotated or negative.
The three most common causes are:
- Metatarsus adductus — the front part of the foot curves inward.
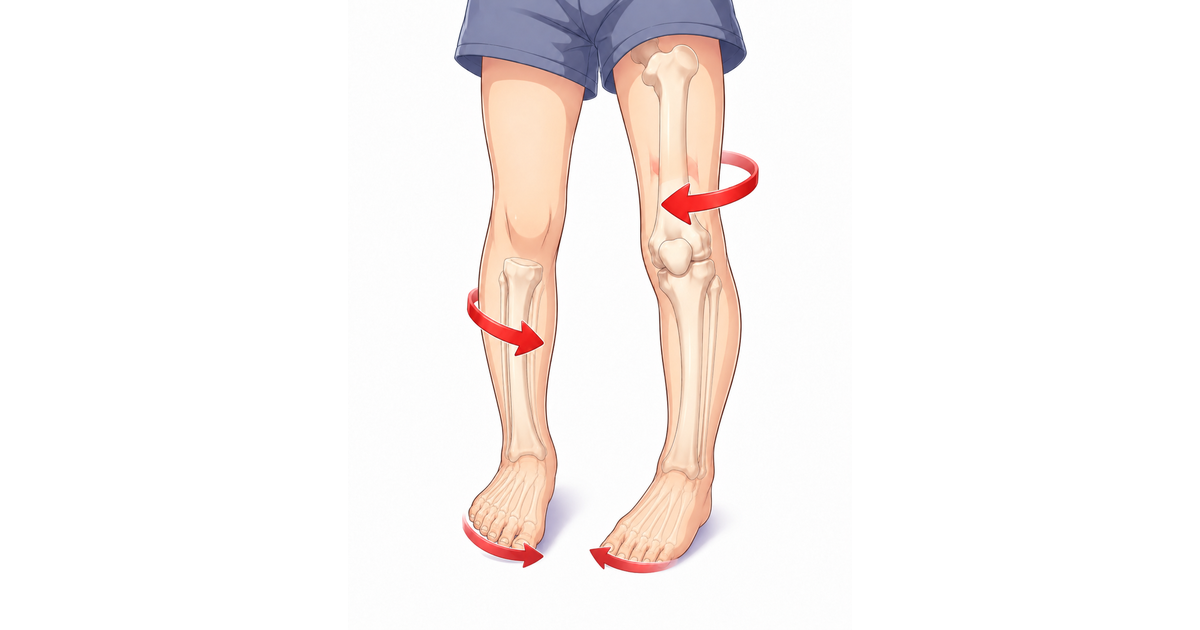
- Internal tibial torsion — the shin bone turns inward.
- Femoral anteversion — the thigh bone/hip turns inward.
AAOS describes these three causes as the main reasons children intoe: the foot turns inward, the shin bone turns inward, or the thigh bone turns inward.
The underlying cause dictates how intoeing is managed.
2. Is intoeing dangerous?
In most children, intoeing is not dangerous. Many cases improve naturally as the child grows. AAOS notes that most young children with intoeing improve without casts, braces, surgery, or special treatment. However, “it usually improves” does not mean every case should be ignored (which happens frequently). Some children have:
- frequent tripping;
- poor confidence when running;
- difficulty in sport;
- unusual shoe wear;
- one side much worse than the other;
- pain;
- limping;
- developmental delay;
- a rigid foot deformity;
- a worsening rather than improving gait.
3. The three main causes of intoeing
A. Metatarsus adductus: when the front of the foot curves inward
Metatarsus adductus is usually seen in babies and young children. The front part of the foot curves inward, giving the foot a C-shaped appearance. Parents may notice that the outer border of the foot looks curved.
This is often thought to be related to the baby’s position in the womb. Many cases are flexible and improve with growth. In a systematic review, Williams and colleagues found strong evidence supporting no treatment for flexible metatarsus adductus, while evidence for treatment was more relevant in semi-rigid or resistant cases.
Flexible | The front of the foot can easily be moved back to a normal position
Semi-flexible | The foot can be corrected to neutral but not beyond
Rigid | The foot cannot be corrected fully by hand
Semi-flexible | The foot can be corrected to neutral but not beyond
Rigid | The foot cannot be corrected fully by hand
Flexible cases usually need monitoring rather than aggressive treatment. More rigid cases may need intervention, especially if they persist.
For flexible metatarsus adductus, observation is often enough.
For more resistant cases, serial casting or orthotic bracing may be used. A randomized trial comparing serial casting with orthosis for resistant metatarsus adductus found that both approaches can improve the deformity.
For more resistant cases, serial casting or orthotic bracing may be used. A randomized trial comparing serial casting with orthosis for resistant metatarsus adductus found that both approaches can improve the deformity.
B. Internal tibial torsion: when the shin bone turns inward
Internal tibial torsion is common in toddlers. Parents often notice that the feet point inward when the child walks, but the kneecaps may still face mostly forward. This suggests that the inward rotation is coming from the shin bone rather than the hip.
AAOS describes tibial torsion as a twisting of the shin bone that causes the feet to turn inward, and Mass General notes that it is often first seen when children start walking and is common between ages 2 and 4.
Internal tibial torsion often improves as the child grows.
What treatment usually involves
For a typical healthy toddler with internal tibial torsion, treatment usually begins with:
- explanation and reassurance;
- measuring and documenting the rotation;
- monitoring over time;
- checking whether the child is tripping or functionally affected.
Routine external braces, splints, special shoes, and heavy bracing are generally not recommended for typical uncomplicated cases. AAOS states that splints, special shoes, and exercise programs do not help tibial torsion.
But this does not mean nothing can be done. If the child is tripping, unstable, or functionally struggling, a discreet in-shoe gait plate can be prescribed.
C. Femoral anteversion: when the thigh bone or hip turns inward
Femoral anteversion usually becomes more obvious in preschool or early school-age children. The child may walk with both knees and feet turned inward. Parents may also notice W-sitting, awkward running, or frequent tripping.
Femoral anteversion means the upper thigh bone is rotated inward more than usual. As a result, the hip naturally rests in more internal rotation.
Femoral anteversion often improves gradually during growth. In a prospective study following children with intoeing until at least age 15, Svenningsen and colleagues found that femoral anteversion decreased over time, with the mean angle reducing from 42° at the first examination to 28° at final follow-up.
Femoral anteversion is not usually “fixed” by forcing the foot straight. The inward rotation comes from higher up at the hip. That is why bulky braces or forceful devices are usually not appropriate for ordinary cases.
However, some children with femoral anteversion trip often or feel embarrassed by the way they walk. In those cases, treatment can focus on functional improvement, not pretending to permanently twist the thigh bone straight.
4. When should parents be concerned?
Most intoeing is benign, but some signs should prompt a more urgent assessment.
Parents should seek professional evaluation if there is:
- pain;
- limping;
- swelling;
- one side much worse than the other;
- worsening over time;
- delayed walking or developmental delay;
- frequent falling that affects school or sport;
- rigid foot deformity;
- neurological signs;
- a history of trauma;
- intoeing associated with weakness or abnormal muscle tone.
AAOS advises that intoeing associated with pain, swelling, or limping should be evaluated.
5. How intoeing should be assessed properly
A good assessment should not simply look at the feet. It should examine the whole lower limb.
A. Walking assessment
The clinician should observe:
- whether one or both feet turn inward;
- whether the knees also turn inward;
- whether the child trips;
- whether running makes it worse;
- whether the child crosses the feet over midline;
- whether the gait is symmetrical;
- whether the child compensates by swinging the leg outward.
B. Foot assessment
This checks for:
- metatarsus adductus;
- flat feet;
- forefoot shape;
- shoe wear;
- flexibility of the foot;
- whether the heel is stable.
C. Tibial rotation assessment
The clinician may measure the thigh-foot angle. This helps determine whether the shin bone is internally rotated.
D. Hip rotation assessment
The clinician checks how far the hips rotate inward and outward. Excessive inward hip rotation with limited outward rotation suggests femoral anteversion.
E. Functional assessment
This is especially important. A child may have a mild-looking intoeing angle but significant tripping, or a larger angle but no symptoms. Treatment decisions should not be based on appearance alone.
6. The treatment philosophy: discreet, functional, child-friendly care
The goal of nonsurgical management is not to frighten parents or overmedicalize normal development. The goal is to help the child function well while growth continues.
A sensible plan should aim to:
- improve walking confidence;
- reduce tripping;
- support participation in school and sport;
- avoid unnecessary visible braces;
- avoid treatment that makes the child feel different;
- minimize disruption to school schedules;
- use low-burden options first;
- monitor progress with objective measurements.
This is where gait plates can be very useful in selected children.
7. Why gait plates are often preferable to external AFO-type braces in mild to moderate idiopathic intoeing
A gait plate is a special type of in-shoe orthotic device designed to influence how the foot moves during walking. It is worn inside normal shoes. Unlike external braces, it is not usually visible. This matters because children are not just small adults. Treatment must consider school, sport, confidence, comfort, and social wellbeing. There are multiple clinics in Singapore and the region that prescribe external AFO-type braces for intoeing. I have spoken out against this and discouraged it.
Gait plates are not over-the-counter insoles. Gait plates are not available in pharmacies. Proper effective gait plates are custom made devices with a peculiar shape that needs to be very accurately designed (stiffness, length, shape). An incorrectly designed gait plate will not have the same result as one manufactured in an experienced podiatric orthotics laboratory.
Gait plates are not over-the-counter insoles. Gait plates are not available in pharmacies. Proper effective gait plates are custom made devices with a peculiar shape that needs to be very accurately designed (stiffness, length, shape). An incorrectly designed gait plate will not have the same result as one manufactured in an experienced podiatric orthotics laboratory.
Advantages of gait plates
1. They are discreet
Gait plates sit inside the shoe. Other children usually cannot see them. This can be important for a child who is self-conscious or does not want to appear different.
2. They fit into normal school life
A gait plate can usually be used in ordinary school shoes or trainers. It does not normally require a child to wear a large external brace.
3. They are less disruptive
Children with busy school schedules, sports, homework, and family routines may struggle with repeated therapy sessions or bulky bracing programs. A gait plate is generally easier to integrate into daily life.
4. They can help gait function
The evidence suggests that gait plates may improve intoeing angle and reduce symptoms in some children. Redmond found that gait plate inlays produced a small but statistically significant reduction in intoeing, and parents reported reduced tripping in 14 of 18 cases.
5. They may improve gait appearance
Ganjehie and colleagues studied children aged 4–10 with intoeing due to excessive femoral anteversion and found that gait plate insoles with shoes increased the angle of gait by 11.1°, compared with 3.85° for shoes alone.
6. They are a reasonable middle ground
For many children, the choice should not be between “do nothing” and “wear a bulky brace.” A gait plate can be a practical middle option for children who are symptomatic but do not require aggressive bracing.
8. What gait plates can and cannot do
Gait plates may help:
- guide the foot into a better walking angle;
- reduce tripping in some children;
- improve visible gait appearance;
- improve confidence during walking and running;
- support the child during natural growth;
- provide a discreet treatment option.
Gait plates should not be presented as magic devices that:
- permanently untwist the thigh bone;
- permanently untwist the shin bone;
- guarantee full correction;
- work for every child;
- replace proper assessment.
9. What about AFO braces?
An AFO, or ankle-foot orthosis, is a larger external brace that supports the ankle and foot. AFOs have an important place in paediatric care when a child has neurological or structural problems such as cerebral palsy, muscle weakness, foot drop, significant instability, or abnormal muscle tone.
However, for ordinary mild to moderate idiopathic intoeing in an otherwise healthy child, AFO-type braces are often excessive. They are more visible, more restrictive, and may interfere with normal footwear and school activities.
AAOS notes that splints, special shoes, and exercise programs do not help typical tibial torsion, and orthopaedic reviews generally advise against traditional bracing for uncomplicated internal tibial torsion and femoral anteversion.
That does not mean braces are never used. It means they should be reserved for the right diagnosis.
When an AFO may be appropriate
An AFO may be considered if there is:
- cerebral palsy;
- abnormal muscle tone;
- foot drop;
- significant ankle instability;
- neurological disease;
- marked weakness;
- a complex gait disorder;
- severe functional impairment requiring more control than an in-shoe device can provide.
For the otherwise healthy child with intoeing, a gait plate is usually a more child-friendly starting point when treatment is needed.
10. Are therapy sessions necessary?
Physiotherapy can be useful in selected children, especially when there is poor balance, weakness, delayed coordination, low tone, poor motor control, or frequent falls.
However, therapy should be realistic. Exercises do not usually change the bony shape of the thigh bone or shin bone. Therapy may help the child move better, become stronger, and coordinate better, but it should not be presented as a guaranteed way to “correct” femoral anteversion or tibial torsion.
For many busy families, repeated therapy appointments can become stressful and difficult to maintain. A practical approach may be:
- assess the child properly;
- use a gait plate if appropriate;
- give a simple home-based strengthening or balance plan;
- monitor progress;
- only add regular therapy if there is a clear functional need.
This avoids overwhelming the child and family.
11. Shoes matter, but shoes alone are not the full treatment
Good shoes can help make walking more stable. They may not correct the cause of intoeing, but they can reduce slipping, instability, and fatigue.
Parents should look for:
- a firm heel counter;
- secure fastening such as laces, Velcro, or straps;
- adequate width;
- enough toe space;
- a sole that is not excessively soft or unstable;
- shoes that are not too large.
Oversized shoes can make tripping worse. Very soft, unstable shoes may also make the child’s gait look more awkward.
In the Ganjehie study, shoes alone improved the angle of gait by 3.85°, while gait plate insoles with shoes improved it by 11.1°, suggesting that footwear can help but that the gait plate had a larger effect in that study.
12. How progress should be monitored
Progress should be measured, not guessed.
A good monitoring plan may include:
- foot progression angle during walking;
- thigh-foot angle;
- hip rotation range;
- frequency of tripping;
- shoe wear pattern;
- parent observations;
- running gait;
- video gait analysis;
- pressure mapping if available;
- comparison over time.
Parents should be told what is being monitored. This gives reassurance and avoids the feeling that treatment is vague.
13. Frequently asked questions:
Will my child grow out of intoeing?
Many children do improve naturally, especially those with internal tibial torsion or femoral anteversion. However, the rate of improvement varies. If your child is tripping, worsening, or one side is much more affected, an assessment is worthwhile.
Is intoeing caused by sitting in the W position?
W-sitting is commonly seen in children with increased femoral anteversion because their hips naturally rotate inward. Parents can encourage other sitting positions, but simply stopping W-sitting does not always correct intoeing.Do gait plates really work?
In selected children, gait plates can help. Studies have shown improvements in foot progression angle and reduced tripping in some children. Redmond reported reduced tripping in 14 of 18 children after gait plate use, while Ganjehie found a larger improvement in angle of gait with gait plates plus shoes compared with shoes alone.
Are gait plates visible?
Are gait plates visible?
Usually, no. They fit inside the child’s shoes, which makes them much less visible than external braces.
Are AFO braces better because they look stronger?
Not necessarily. A stronger-looking device is not always better. For ordinary idiopathic intoeing, large braces may be unnecessary and burdensome. AFOs are more appropriate for neurological or more complex gait problems.
Can exercises correct intoeing?
Exercises can help strength, balance, and coordination. They usually do not change the bony rotation of the thigh bone or shin bone. Therapy should be used when there is a clear functional reason, not as a stressful routine with unrealistic promises.
When is surgery needed?
Surgery is rare. It is usually considered only in older children with severe persistent deformity and significant functional problems. Most children never need surgery.
14. Summary
Intoeing is common. It usually comes from one of three places: the foot, the shin bone, or the hip. Many children improve naturally, but some children need help because they trip, struggle with sport, walk awkwardly, or become self-conscious.
For those children, treatment should be practical and child-friendly. Correctly prescribed and manufactured gait plates are often a sensible option because they are discreet, fit inside normal shoes, and can improve walking angle and tripping in selected cases. They are usually far less disruptive than external AFO-type braces and less demanding than repeated therapy sessions.
The best care is not about forcing every child into treatment. It is about careful assessment, honest explanation, objective monitoring, and choosing the least disruptive option that helps the child move better.
Not every doctor has sufficient knowledge and experience with intoeing. Not every clinic that claims to treat intoeing has the proper laboratory facilities to manufacture gait plates either. Selecting the correct clinician is part of the intoeing treatment journey for your child. Since management of this condition may take a few years, it is important to make an informed decision.
Book An Appointment
Disclaimer: The word "treatment" in this article refers to the care and management of a patient’s health to prevent, cure, or improve a condition. Treatment results vary and do not necessarily indicate a cure. This article is for informational and educational purposes only and does not constitute medical advice.
About the author
Mark Reyneker is a podiatrist and human gait specialist with 8 years of training and over 25 years of clinical experience. He is the Founder and Clinical Director of Family Podiatry Centre and has a Bachelors degree in Podiatric Medicine and a Master’s degree in paleoanthropology, with research focused on human foot function and metatarsal loading.
Social Media Link
Not every doctor has sufficient knowledge and experience with intoeing. Not every clinic that claims to treat intoeing has the proper laboratory facilities to manufacture gait plates either. Selecting the correct clinician is part of the intoeing treatment journey for your child. Since management of this condition may take a few years, it is important to make an informed decision.
Book An Appointment
Disclaimer: The word "treatment" in this article refers to the care and management of a patient’s health to prevent, cure, or improve a condition. Treatment results vary and do not necessarily indicate a cure. This article is for informational and educational purposes only and does not constitute medical advice.
About the author
Mark Reyneker is a podiatrist and human gait specialist with 8 years of training and over 25 years of clinical experience. He is the Founder and Clinical Director of Family Podiatry Centre and has a Bachelors degree in Podiatric Medicine and a Master’s degree in paleoanthropology, with research focused on human foot function and metatarsal loading.
Social Media Link